

Evaluating the Age-Based Recommendations for Long-Term Follow-Up in Breast Cancer
- PMID: 32510767
- PMCID: PMC7485372
- DOI: 10.1634/theoncologist.2019-0973
Evaluating the Age-Based Recommendations for Long-Term Follow-Up in Breast Cancer
Abstract
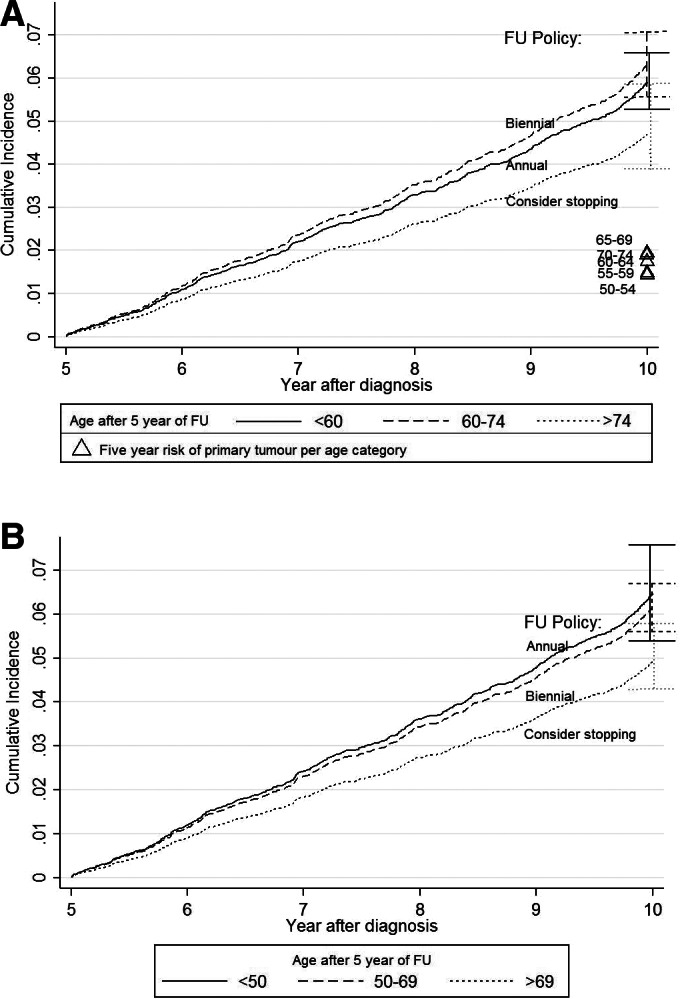
Background: After 5 years of annual follow-up following breast cancer, Dutch guidelines are age based: annual follow-up for women <60 years, 60-75 years biennial, and none for >75 years. We determined how the risk of recurrence corresponds to these consensus-based recommendations and to the risk of primary breast cancer in the general screening population.
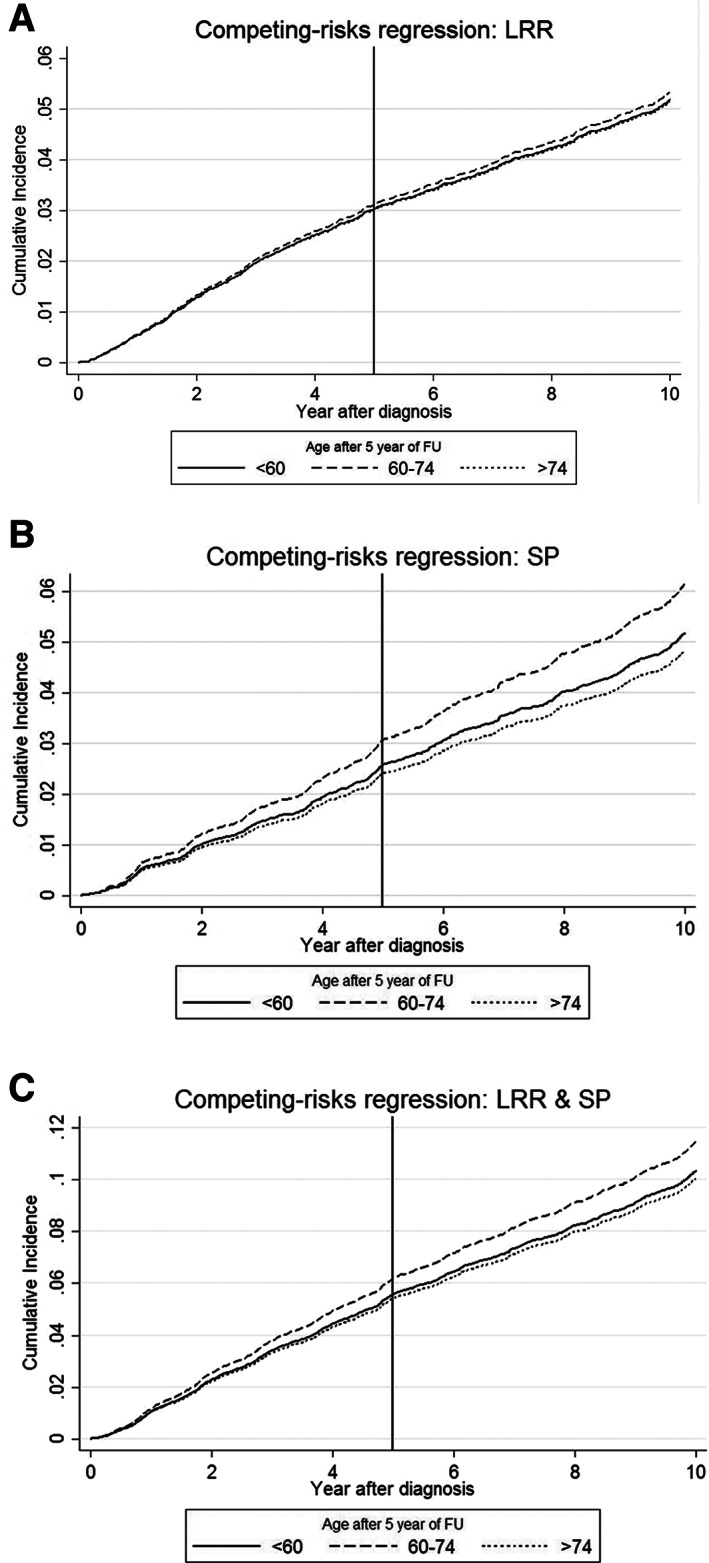
Subjects, materials, and methods: Women with early-stage breast cancer in 2003/2005 were selected from the Netherlands Cancer Registry (n = 18,568). Cumulative incidence functions were estimated for follow-up years 5-10 for locoregional recurrences (LRRs) and second primary tumors (SPs). Risks were compared with the screening population without history of breast cancer. Alternative cutoffs for age were determined by log-rank tests.
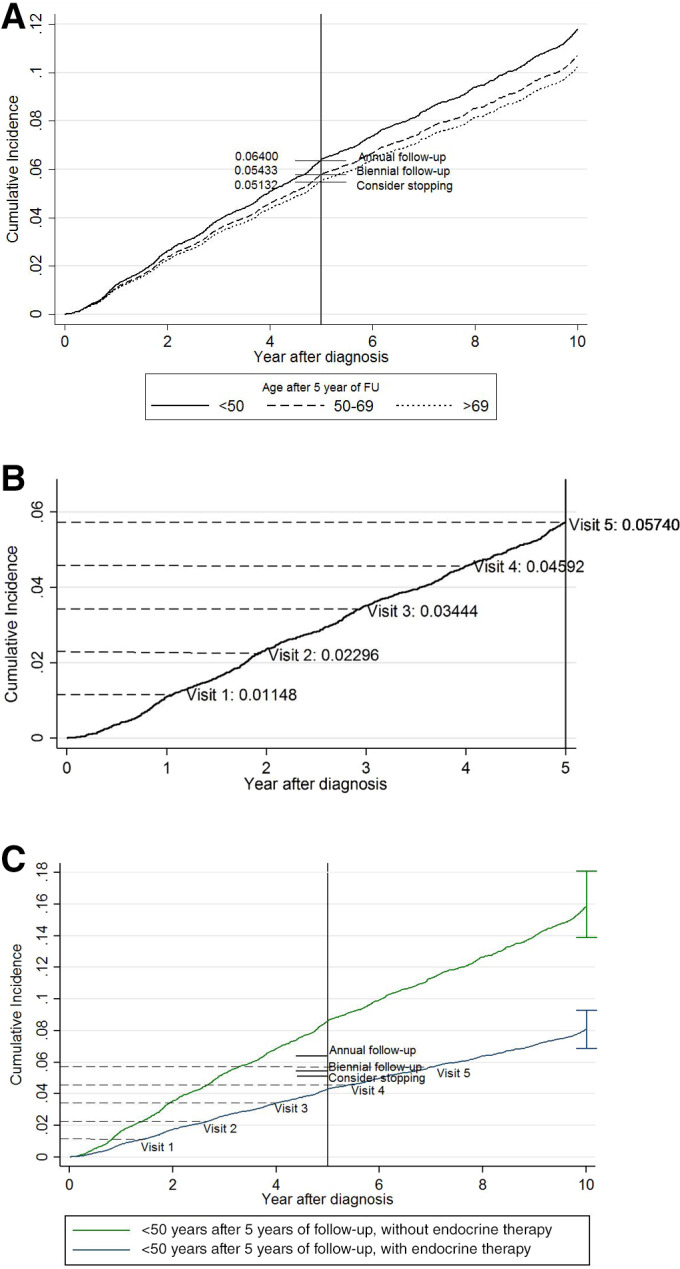
Results: The cumulative risk for LRR/SP was lower in women <60 years (5.9%, 95% confidence interval [CI] 5.3-6.6) who are under annual follow-up than for women 60-75 (6.3%, 95% CI 5.6-7.1) receiving biennial visits. All risks were higher than the 5-year risk of a primary tumor in the screening population (ranging from 1.4% to 1.9%). Age cutoffs <50, 50-69, and > 69 revealed better risk differentiation and would provide more risk-based schedules. Still, other factors, including systemic treatments, had an even greater impact on recurrence risks.
Conclusion: The current consensus-based recommendations use suboptimal age cutoffs. The proposed alternative cutoffs will lead to a more balanced risk-based follow-up and thereby more efficient allocation of resources. However, more factors should be taken into account for truly individualizing follow-up based on risk for recurrence.
Implications for practice: The current age-based recommendations for breast cancer follow-up after 5 years are suboptimal and do not reflect the actual risk of recurrent disease. This results in situations in which women with higher risks actually receive less follow-up than those with a lower risk of recurrence. Alternative cutoffs could be a start toward risk-based follow-up and thereby more efficient allocation of resources. However, age, or any single risk factor, is not able to capture the risk differences and therefore is not sufficient for determining follow-up. More risk factors should be taken into account for truly individualizing follow-up based on the risk for recurrence.
Keywords: Breast cancer; Locoregional recurrence; Risk-based follow-up; Second primary; Thresholds.
© 2020 The Authors. The Oncologist published by Wiley Periodicals LLC on behalf of AlphaMed Press.
Conflict of interest statement
Figures
References
-
- Grandjean I, Kwast ABG, de Vries H et al. Evaluation of the adherence to follow‐up care guidelines for women with breast cancer. Eur J Oncol Nurs 2012;16:281–285. - PubMed
-
- Runowicz CD, Leach CR, Henry NL et al. American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline. CA Cancer J Clin 2016;66:43–73. - PubMed
-
- Netherlands Comprehensive Cancer Organisation (IKNL) (2012) Dutch breast cancer guideline. Available at http://www.oncoline.nl/breastcancer. Accessed March 2, 2019.
-
- Rosselli MDT, Cariddi A. Intensive diagnostic follow‐up after treatment of primary breast cancer. A randomized trial. J Am Med Assoc 1994;271:1593–1597. - PubMed
-
- Geurts SME, De Vegt F, Siesling S et al. Pattern of follow‐up care and early relapse detection in breast cancer patients. Breast Cancer Res Treat 2012;136:859–868. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
