

Cognitive Impairment among Veterans in Outpatient Vision Rehabilitation
- PMID: 32511169
- PMCID: PMC7291825
- DOI: 10.1097/OPX.0000000000001522
Cognitive Impairment among Veterans in Outpatient Vision Rehabilitation
Abstract
Significance: Outpatient vision rehabilitation improves function in veterans with vision impairment, but the prevalence of cognitive impairment and the degree to which it may affect rehabilitation outcomes in the Veterans Affairs system are unknown.
Purpose: The purpose of this study was to determine the prevalence of cognitive impairment among veterans receiving outpatient vision rehabilitation in the Veterans Affairs system and compare the benefits of rehabilitation in veterans with and without cognitive impairment.
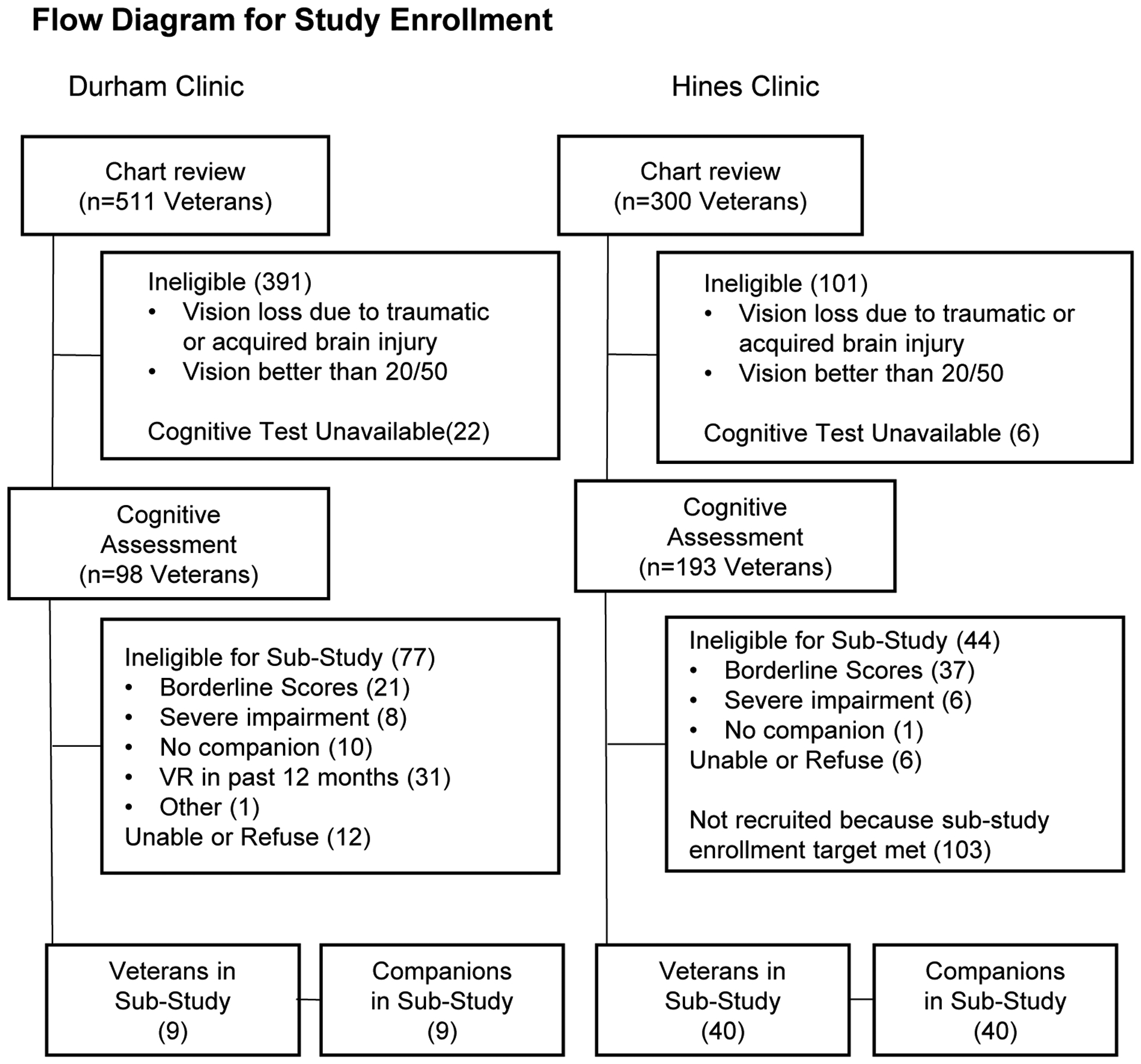
Methods: We conducted cognitive assessments and a nested longitudinal cohort study in veterans with eye disorders at two outpatient rehabilitation sites. Cognition was assessed with the Modified Telephone Interview for Cognitive Status administered in person. Eligible veterans and their companions in the longitudinal study responded to questions about the veteran's function at baseline and 90 days later. Visual function was measured with the 48-item Low Vision Visual Function Questionnaire (LV-VFQ-48) and items from the Activity Inventory.
Results: Of 291 veterans assessed (mean ± standard deviation age, 78.2 ± 12 years), 136 (46.7%) were cognitively intact (Modified Telephone Interview for Cognitive Status scores, ≥33), whereas 58 (19.9%) had borderline scores of 30 to 32, 82 (28.2%) had scores suggesting mild/moderate cognitive impairment (scores of 20 to 29), and 15 (5.2%) had scores suggesting severe cognitive impairment (score of <20). After 90 days, mean LV-VFQ-48 reading scores tended to improve in veterans with (n = 21) and without (n = 28) cognitive impairment. The magnitude of self-reported improvement in LV-VFQ-48 scores was greater among cognitively intact, compared with cognitively impaired, veterans (effect size, 0.56 for reading; 0.71 for visual motor). Veterans and companions reported similar 90-day reduction in difficulty with the veterans' top 3 Activity Inventory goals, regardless of cognitive status.
Conclusions: Approximately one in three veterans referred to outpatient vision rehabilitation has detectable cognitive impairment, yet many still experience functional improvements. Future research should determine best practices to accommodate challenges associated with cognitive impairment in vision rehabilitation and to track clinically meaningful outcomes.
Figures

References
-
- Massof RW, Dagnelie G, Deremik JT. Low Vision Rehabilitation in the U.S. Health Care System. J Vis Rehabil 1995;9:3–25.
-
- National Academies of Medicine. Making Eye Health a Population Health Imperative: Vision for Tomorrow. Washington DC: National Academies Press; 2016. - PubMed
-
- Renieri G, Pitz S, Pfeiffer N, et al. Changes in Quality of Life in Visually Impaired Patients after Low-Vision Rehabilitation. Int J Rehabil Res 2013;36:48–55. - PubMed
-
- Wang BZ, Pesudovs K, Keane MC, et al. Evaluating the Effectiveness of Multidisciplinary Low-Vision Rehabilitation. Optom Vis Sci 2012;89:1399–408. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
