

This is a preprint.
Covid-19 by Race and Ethnicity: A National Cohort Study of 6 Million United States Veterans
- PMID: 32511524
- PMCID: PMC7273292
- DOI: 10.1101/2020.05.12.20099135
Covid-19 by Race and Ethnicity: A National Cohort Study of 6 Million United States Veterans
Update in
-
Patterns of COVID-19 testing and mortality by race and ethnicity among United States veterans: A nationwide cohort study.PLoS Med. 2020 Sep 22;17(9):e1003379. doi: 10.1371/journal.pmed.1003379. eCollection 2020 Sep. PLoS Med. 2020. PMID: 32960880 Free PMC article.
Abstract
Background: There is growing concern that racial and ethnic minority communities around the world are experiencing a disproportionate burden of morbidity and mortality from symptomatic SARS-Cov-2 infection or coronavirus disease 2019 (Covid-19). Most studies investigating racial and ethnic disparities to date have focused on hospitalized patients or have not characterized who received testing or those who tested positive for Covid-19.
Objective: To compare patterns of testing and test results for coronavirus 2019 (Covid-19) and subsequent mortality by race and ethnicity in the largest integrated healthcare system in the United States.
Design: Retrospective cohort study.
Setting: United States Department of Veterans Affairs (VA).
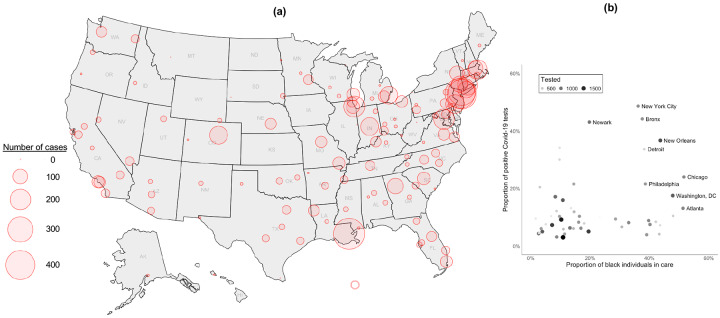
Participants: 5,834,543 individuals in care, among whom 62,098 were tested and 5,630 tested positive for Covid-19 between February 8 and May 4, 2020. Exposures: Self-reported race/ethnicity.
Main outcome measures: We evaluated associations between race/ethnicity and receipt of Covid-19 testing, a positive test result, and 30-day mortality, accounting for a wide range of demographic and clinical risk factors including comorbid conditions, site of care, and urban versus rural residence.
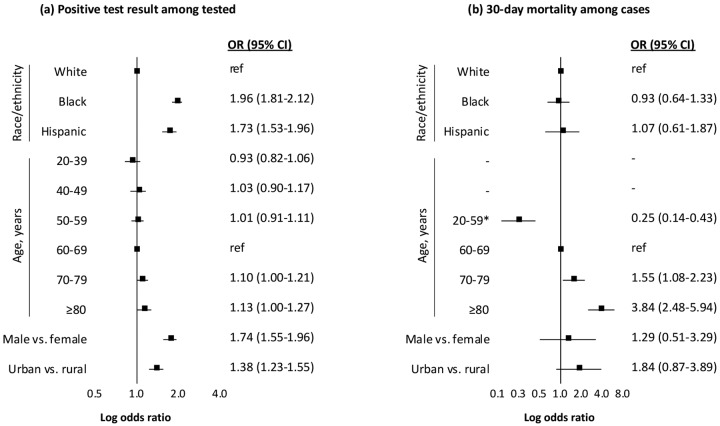
Results: Among all individuals in care, 74% were non-Hispanic white (white), 19% non-Hispanic black (black), and 7% Hispanic. Compared with white individuals, black and Hispanic individuals were more likely to be tested for Covid-19 (tests per 1000: white=9.0, [95% CI 8.9 to 9.1]; black=16.4, [16.2 to 16.7]; and Hispanic=12.2, [11.9 to 12.5]). While individuals from minority backgrounds were more likely to test positive (black vs white: OR 1.96, 95% CI 1.81 to 2.12; Hispanic vs white: OR 1.73, 95% CI 1.53 to 1.96), 30-day mortality did not differ by race/ethnicity (black vs white: OR 0.93, 95% CI 0.64 to 1.33; Hispanic vs white: OR 1.07, 95% CI 0.61 to 1.87).
Conclusions: Black and Hispanic individuals are experiencing an excess burden of Covid-19 not entirely explained by underlying medical conditions or where they live or receive care. While there was no observed difference in mortality by race or ethnicity, our findings may underestimate risk in the broader US population as health disparities tend to be reduced in VA.
Conflict of interest statement
Conflicts of interest
All authors have completed the ICMJE Unified Competing Interest form (available on request from the corresponding author) and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. In summary, the authors declare no conflicts of interest.
Figures
References
-
- Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. COVID-19 Dashboard, 2020:https://coronavirus.jhu.edu/map.html.
-
- Reyes C, Husain N, Gutowski C, et al. Chicago’s coronavirus disparity: Black Chicagoans are dying at nearly six times the rate of white residents, data show. Chicago: Tribune; April 7, 2020.
-
- Thebault R, Tran A, Williams V. The coronavirus is infecting and killing black Americans at an alarmingly high rate. The Washington Post April 7, 2020.
-
- Deslatte M. Louisiana data: virus hits blacks, people with hypertension. AP News April 7, 2020.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous