

Special Article - Acute myocardial injury in patients hospitalized with COVID-19 infection: A review
- PMID: 32512122
- PMCID: PMC7274977
- DOI: 10.1016/j.pcad.2020.05.013
Special Article - Acute myocardial injury in patients hospitalized with COVID-19 infection: A review
Abstract
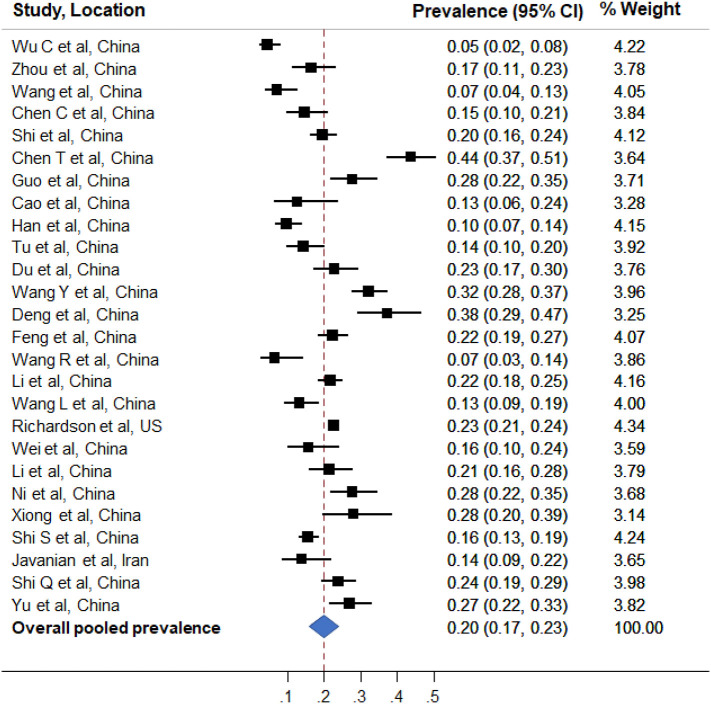
The Coronavirus Disease 2019 (COVID-19) is now a global pandemic with millions affected and millions more at risk for contracting the infection. The COVID-19 virus, SARS-CoV-2, affects multiple organ systems, especially the lungs and heart. Elevation of cardiac biomarkers, particularly high-sensitivity troponin and/or creatine kinase MB, is common in patients with COVID-19 infection. In our review of clinical analyses, we found that in 26 studies including 11,685 patients, the weighted pooled prevalence of acute myocardial injury was 20% (ranged from 5% to 38% depending on the criteria used). The plausible mechanisms of myocardial injury include, 1) hyperinflammation and cytokine storm mediated through pathologic T-cells and monocytes leading to myocarditis, 2) respiratory failure and hypoxemia resulting in damage to cardiac myocytes, 3) down regulation of ACE2 expression and subsequent protective signaling pathways in cardiac myocytes, 4) hypercoagulability and development of coronary microvascular thrombosis, 5) diffuse endothelial injury and 'endotheliitis' in several organs including the heart, and, 6) inflammation and/or stress causing coronary plaque rupture or supply-demand mismatch leading to myocardial ischemia/infarction. Cardiac biomarkers can be used to aid in diagnosis as well as risk stratification. In patients with elevated hs-troponin, clinical context is important and myocarditis as well as stress induced cardiomyopathy should be considered in the differential, along with type I and type II myocardial infarction. Irrespective of etiology, patients with acute myocardial injury should be prioritized for treatment. Clinical decisions including interventions should be individualized and carefully tailored after thorough review of risks/benefits. Given the complex interplay of SARS-CoV-2 with the cardiovascular system, further investigation into potential mechanisms is needed to guide effective therapies. Randomized trials are urgently needed to investigate treatment modalities to reduce the incidence and mortality associated with COVID-19 related acute myocardial injury.
Keywords: Biomarkers; COVID-19; Management; Myocardial injury; Prognosis.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures

References
-
- Chen C., Chen C., Yan J.T., Zhou N., Zhao J.P., Wang D.W. Analysis of myocardial injury in patients with COVID-19 and association between concomitant cardiovascular diseases and severity of COVID-19. Zhonghua Xin Xue Guan Bing Za Zhi. 2020;48:E008. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
