

Antegrade Intentional Laceration of the Anterior Mitral Leaflet to Prevent Left Ventricular Outflow Tract Obstruction: A Simplified Technique From Bench to Bedside
- PMID: 32513014
- PMCID: PMC7380541
- DOI: 10.1161/CIRCINTERVENTIONS.119.008903
Antegrade Intentional Laceration of the Anterior Mitral Leaflet to Prevent Left Ventricular Outflow Tract Obstruction: A Simplified Technique From Bench to Bedside
Abstract
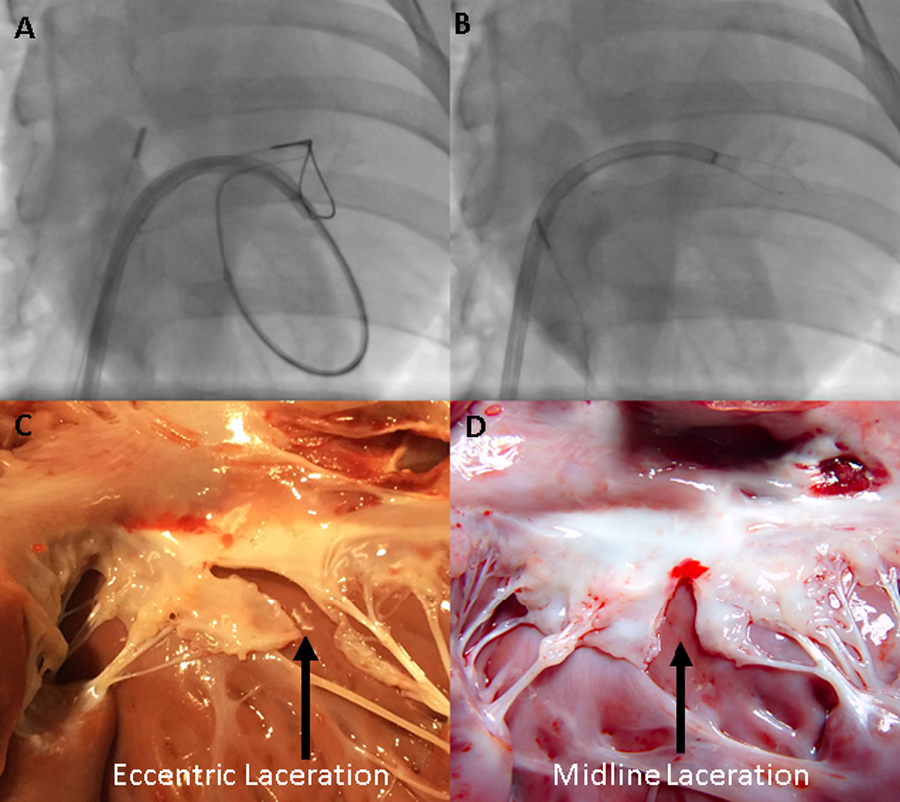
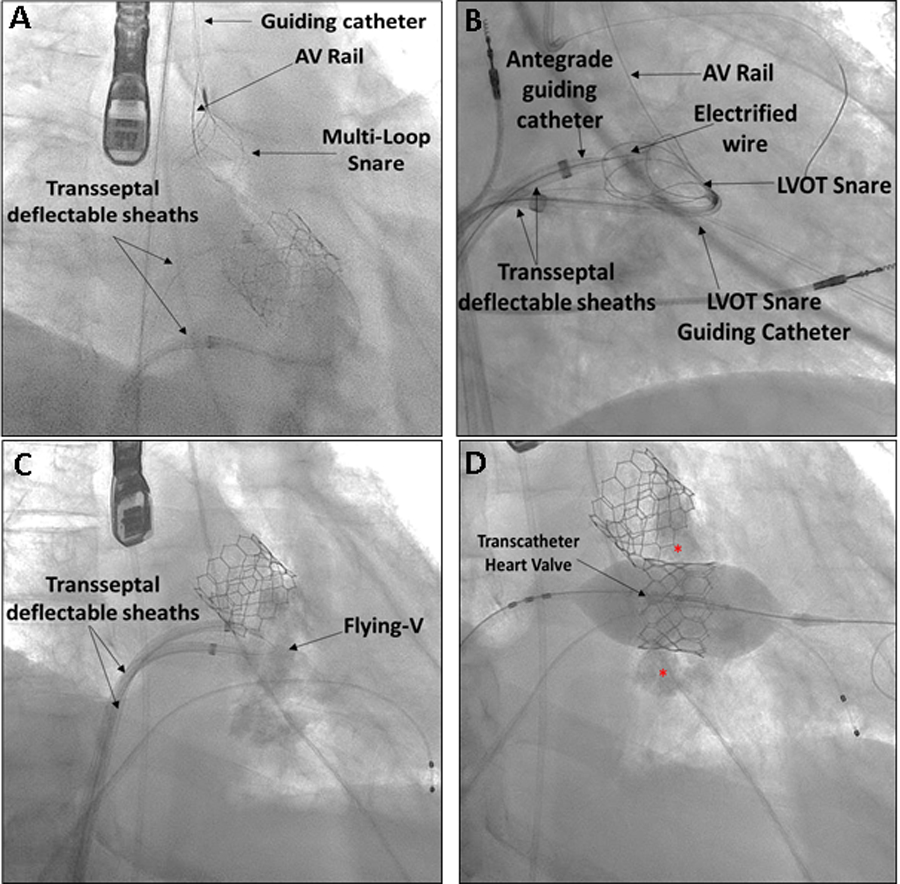
Background: Intentional laceration of the anterior mitral leaflet (LAMPOON) is an effective adjunct to transcatheter mitral valve replacement that prevents left ventricular outflow tract (LVOT) obstruction. To date, LAMPOON has been performed in over 150 patients using a retrograde approach that can be technically challenging. A modified antegrade transseptal technique may simplify the procedure.
Methods: Antegrade LAMPOON was developed and tested in nonsurvival pig experiments. Thereafter, antegrade LAMPOON was performed in patients at prohibitive risk of LVOT obstruction. Clinical, procedural, and angiographic details were abstracted from medical records of their index procedure, and were compared with findings in comparable patients at risk of fixed-LVOT obstruction in the LAMPOON investigational device exemption trial.
Results: Eight patients at risk of fixed LVOT obstruction underwent antegrade LAMPOON. Leaflet traversal and laceration were technically successful in all. There were no cases of clinically significant LVOT obstruction (mean LVOT gradient at discharge: 5.4±1.4 mm Hg). One patient suffered a ventricular wire perforation, unrelated to the antegrade LAMPOON technique, and did not survive to discharge. At the time of discharge, no patients had an increase of >10 mm Hg in LVOT gradient compared with baseline. Procedure times (from traversal to transcatheter mitral valve replacement) were shorter, compared with the retrograde technique in the LAMPOON investigational device exemption trial (39±09 versus 65±35 minutes). All patients survived (8/8, 100%) the procedure, and 7/8 (88%) survived to 30 days, similar to subjects in the LAMPOON investigational device exemption trial.
Conclusions: Antegrade LAMPOON is an effective, reproducible, and simplified strategy to lacerate the anterior leaflet before transcatheter mitral valve replacement. The authors recommend the technique as the new standard for LAMPOON.
Keywords: cardiac catheterization; electrosurgery; heart valve prosthesis implantation; lacerations; mitral valve; tomography, X-ray computed; ventricular outflow obstruction.
Conflict of interest statement
Disclosures
ABG is a proctor for Edwards Lifesciences, Medtronic, and Abbott Vascular. He has an equity interest in Transmural Systems. His employer has research contracts for clinical investigation of transcatheter aortic, mitral, and tricuspid devices from Edwards Lifesciences, Abbott Vascular, Medtronic, and Boston Scientific.
JMK is a proctor for Edwards Lifesciences and Medtronic.
GP is a consultant and proctor for Edwards Lifesciences.
KG is a speaker, proctor, and principle investigator for Edwards Lifesciences. She is a speaker, proctor, and advisory board member for Boston Scientific. She is a speaker, proctor, principle investigator, advisory board member, and national principle investigator for Medtronic.
JMM has received honoraria from Edwards Lifesciences, Boston Scientific, and Teleflex All other authors report no relevant conflict of interest.
TR is a proctor for Edwards Lifesciences and Medtronic.
JMK, RJL, and TR are co-inventors on patents, assigned to the NIH, on devices for electrosurgical leaflet laceration. RJL’s employer received research support from Edwards Lifesciences for transcatheter modification of the mitral valve.
VCB is a consultant for Edwards Lifesciences and Abbott Vascular, and his employer has research contracts for clinical investigation of transcatheter aortic, mitral, and tricuspid devices from Edwards Lifesciences, Abbott Vascular, Medtronic, and Boston Scientific. He has an equity interest in Transmural Systems.
Figures

References
-
- Greenbaum AB, Condado JF, Eng M, Lerakis S, Wang DD, Kim DW, Lederman RJ, Paone G, Neill WWO, Thourani VH, et al. Long or redundant leaflet complicating transcatheter mitral valve replacement: Case vignettes that advocate for removal or reduction of the anterior mitral leaflet. Catheter Cardiovasc Interv 2018;92:627–632. - PMC - PubMed
-
- Guerrero M, Urena M, Himbert D, Wang DD, Eleid M, Kodali S, George I, Chakravarty T, Mathur M, Holzhey D, et al. 1-Year Outcomes of Transcatheter Mitral Valve Replacement in Patients With Severe Mitral Annular Calcification. J Am Coll Cardiol 2018;71:1841–1853. - PubMed
-
- Khan JM, Rogers T, Schenke WH, Mazal JR, Faranesh AZ, Greenbaum AB, Babaliaros VC, Chen MY and Lederman RJ. Intentional Laceration of the Anterior Mitral Valve Leaflet to Prevent Left Ventricular Outflow Tract Obstruction During Transcatheter Mitral Valve Replacement: Pre-Clinical Findings. JACC Cardiovasc Interv 2016;9:1835–43. - PMC - PubMed
-
- Babaliaros VC, Greenbaum AB, Khan JM, Rogers T, Wang DD, Eng MH, O’Neill WW, Paone G, Thourani VH, Lerakis S, et al. Intentional Percutaneous Laceration of the Anterior Mitral Leaflet to Prevent Outflow Obstruction During Transcatheter Mitral Valve Replacement: First-in-Human Experience. JACC Cardiovasc Interv 2017;10:798–809. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
