

Stigma for common mental disorders in racial minorities and majorities a systematic review and meta-analysis
- PMID: 32513215
- PMCID: PMC7278062
- DOI: 10.1186/s12889-020-08964-3
Stigma for common mental disorders in racial minorities and majorities a systematic review and meta-analysis
Erratum in
-
Correction to: Stigma for common mental disorders in racial minorities and majorities a systematic review and meta-analysis.BMC Public Health. 2020 Sep 1;20(1):1326. doi: 10.1186/s12889-020-09199-y. BMC Public Health. 2020. PMID: 32873268 Free PMC article.
Abstract
Background: There is a strong stigma attached to mental disorders preventing those affected from getting psychological help. The consequences of stigma are worse for racial and/or ethnic minorities compared to racial and/or ethnic majorities since the former often experience other social adversities such as poverty and discrimination within policies and institutions. This is the first systematic review and meta-analysis summarizing the evidence on the impact of differences in mental illness stigma between racial minorities and majorities.
Methods: This systematic review and meta-analysis included cross-sectional studies comparing mental illness stigma between racial minorities and majorities. Systematic searches were conducted in the bibliographic databases of PubMed, PsycINFO and EMBASE until 20th December 2018. Outcomes were extracted from published reports, and meta-analyses, and meta-regression analyses were conducted in CMA software.
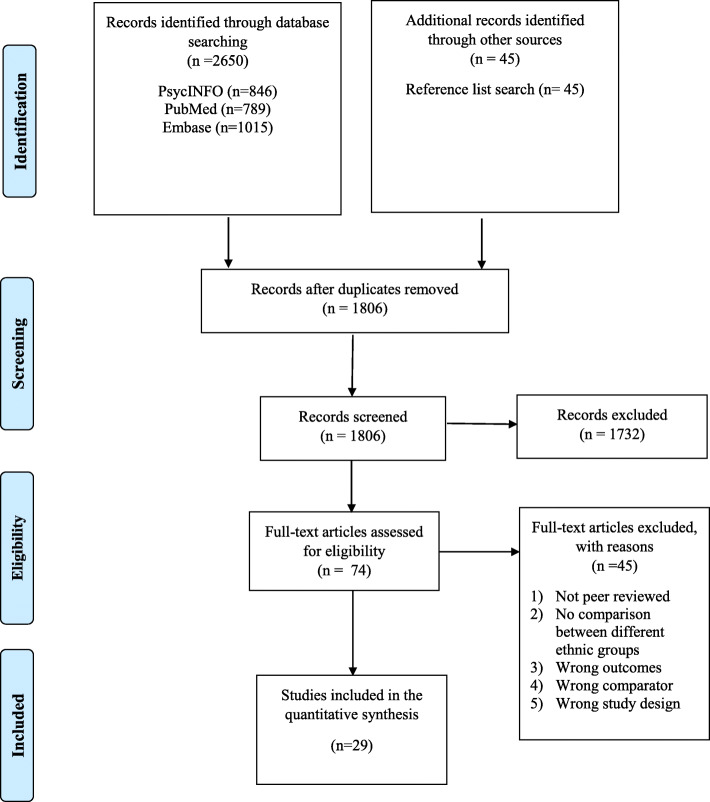
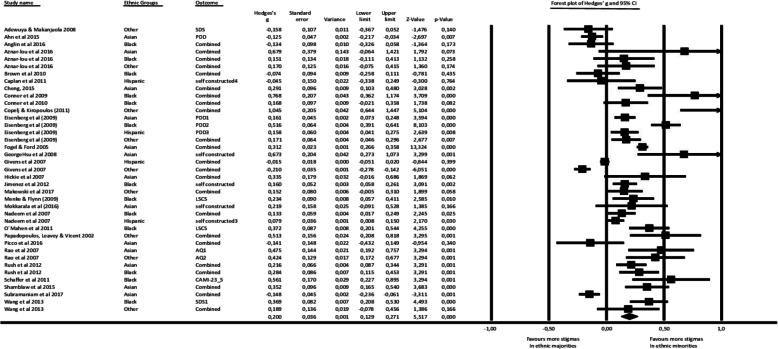
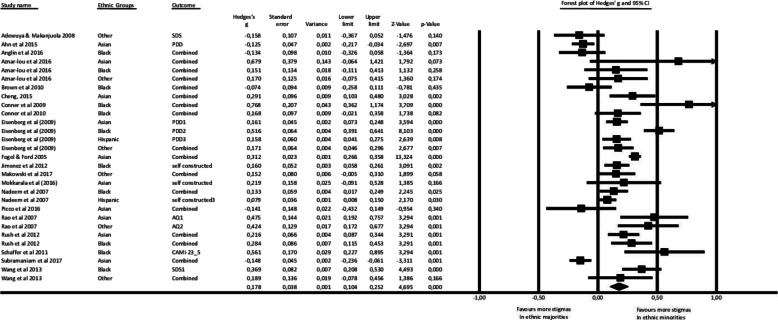
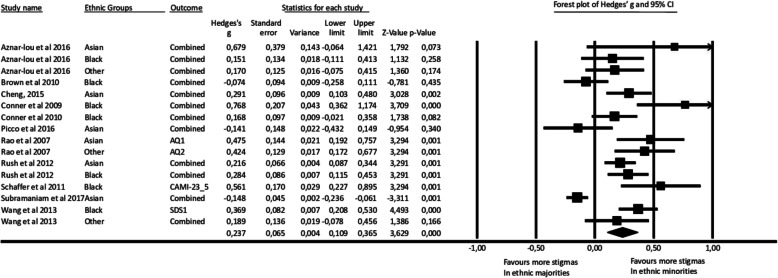
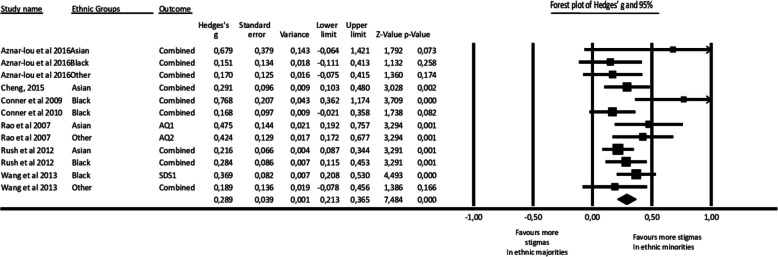
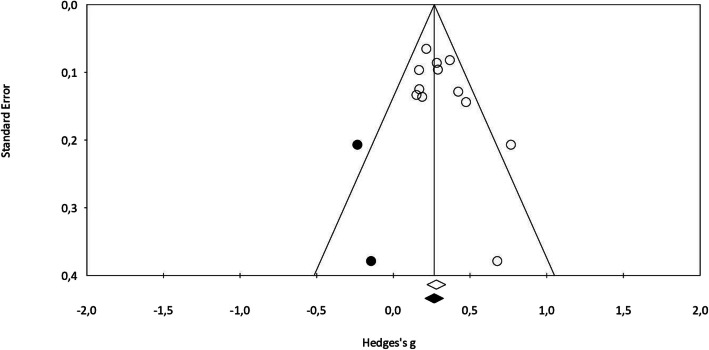
Results: After screening 2787 abstracts, 29 studies with 193,418 participants (N = 35,836 in racial minorities) were eligible for analyses. Racial minorities showed more stigma than racial majorities (g = 0.20 (95% CI: 0.12 ~ 0.27) for common mental disorders. Sensitivity analyses showed robustness of these results. Multivariate meta-regression analyses pointed to the possible moderating role of the number of studies with high risk of bias on the effect size. Racial minorities have more stigma for common mental disorders when compared with majorities. Limitations included moderate to high risk of bias, high heterogeneity, few studies in most comparisons, and the use of non-standardized outcome measures.
Conclusions: Mental illness stigma is higher among ethnic minorities than majorities. An important clinical implication of these findings would be to tailor anti-stigma strategies related with mental illnesses according to specific racial and/or ethnic backgrounds with the intention to improve mental health outreach.
Keywords: Common mental disorders; Mental illness stigma; Racial minorities; Stigma.
Conflict of interest statement
None.
Figures
Similar articles
-
Exploring stigma associated with mental health conditions and alcohol and other drug use among people from migrant and ethnic minority backgrounds: a protocol for a systematic review of qualitative studies.Syst Rev. 2022 Jan 18;11(1):12. doi: 10.1186/s13643-021-01875-3. Syst Rev. 2022. PMID: 35042545 Free PMC article.
-
Racial and ethnic minority college students' stigma associated with seeking psychological help: Examining psychocultural correlates.J Couns Psychol. 2013 Jan;60(1):98-111. doi: 10.1037/a0031169. J Couns Psychol. 2013. PMID: 23356468
-
Systematic Review of Cultural Aspects of Stigma and Mental Illness among Racial and Ethnic Minority Groups in the United States: Implications for Interventions.Am J Community Psychol. 2021 Dec;68(3-4):486-512. doi: 10.1002/ajcp.12516. Epub 2021 Apr 3. Am J Community Psychol. 2021. PMID: 33811676
-
Mental health impacts of racial discrimination in Australian culturally and linguistically diverse communities: a cross-sectional survey.BMC Public Health. 2015 Apr 18;15:401. doi: 10.1186/s12889-015-1661-1. BMC Public Health. 2015. PMID: 25911973 Free PMC article.
-
Peer Support as an Ideal Solution for Racial/Ethnic Disparities in Colorectal Cancer Screening: Evidence from a Systematic Review and Meta-analysis.Dis Colon Rectum. 2020 Jun;63(6):850-858. doi: 10.1097/DCR.0000000000001611. Dis Colon Rectum. 2020. PMID: 32167969
Cited by
-
Language use on Twitter reflects social structure and social disparities.Heliyon. 2023 Dec 12;10(2):e23528. doi: 10.1016/j.heliyon.2023.e23528. eCollection 2024 Jan 30. Heliyon. 2023. PMID: 38293550 Free PMC article.
-
Looking through the lens of stigma: Understanding and anticipating concerns about the responsible development and use of psychiatric electroceutical interventions (PEIs).SSM Ment Health. 2023 Dec 15;4:100261. doi: 10.1016/j.ssmmh.2023.100261. Epub 2023 Sep 6. SSM Ment Health. 2023. PMID: 38188866 Free PMC article.
-
"It's Okay to Not Be Okay": Mental Health Concerns and New Directions as a Result of the COVID-19 Pandemic.Perform Enhanc Health. 2022 Feb;10(1):100218. doi: 10.1016/j.peh.2022.100218. Epub 2022 Jan 19. Perform Enhanc Health. 2022. PMID: 36570049 Free PMC article. No abstract available.
-
Perceived discrimination as a mediator between cultural identity and mental health symptoms among racial/ethnic minority adults in the United States: insights from the Health Information National Trends Survey 6.Front Psychol. 2024 Feb 28;15:1233919. doi: 10.3389/fpsyg.2024.1233919. eCollection 2024. Front Psychol. 2024. PMID: 38481618 Free PMC article.
-
Scope, Findability, and Quality of Information About Music-Based Interventions in Oncology: Quantitative Content Analysis of Public-Facing Websites at National Cancer Institute-Designated Cancer Centers.JMIR Cancer. 2024 Nov 22;10:e53440. doi: 10.2196/53440. JMIR Cancer. 2024. PMID: 39584538 Free PMC article.
References
-
- Ustün TB, Ayuso-Mateos JL, Chatterji S, Mathers C, Murray CJ. Global burden of depressive disorders in the year 2000. Br J Psychiatry. 2004;184:386–92. 10.1192/bjp.184.5.386. - PubMed
-
- Cuijpers P, Munoz RF, Clarke GN, Lewinsohn PM. Psychoeducational treatment and prevention of depression: the "coping with Depression" course thirty years later. Clin Psychol Rev. 2009;29:449–458. - PubMed
-
- Cuijpers P, Eylem O, Karyotaki E, Zhou X, Sijbrandij M. Psychotherapy for depression and anxiety in low- and middle-income countries. In: Stein D, Bass J, editors. Global Mental Health and Psychotherapy: Adapting Psychotherapy for Low- and Middle-Income Countries. Elsevier; 2019. p. 173–92. 10.1016/b978-0-12-814932-4.00008-2.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
