

Reversible suppression of T cell function in the bone marrow microenvironment of acute myeloid leukemia
- PMID: 32513686
- PMCID: PMC7321988
- DOI: 10.1073/pnas.1916206117
Reversible suppression of T cell function in the bone marrow microenvironment of acute myeloid leukemia
Abstract
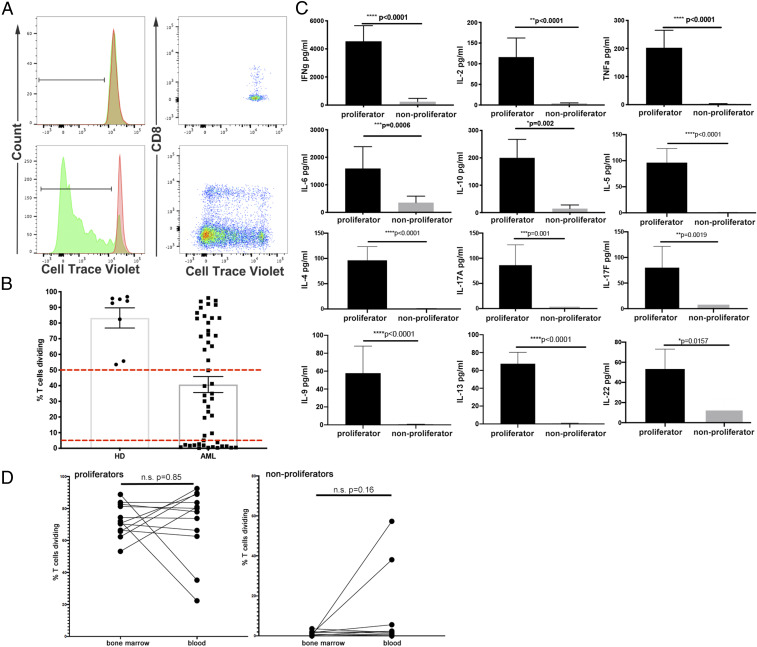
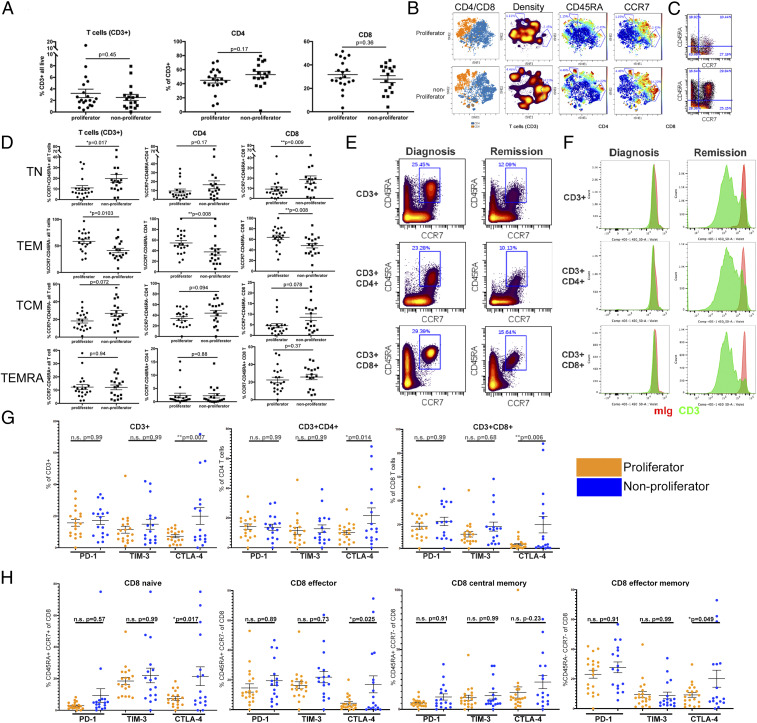
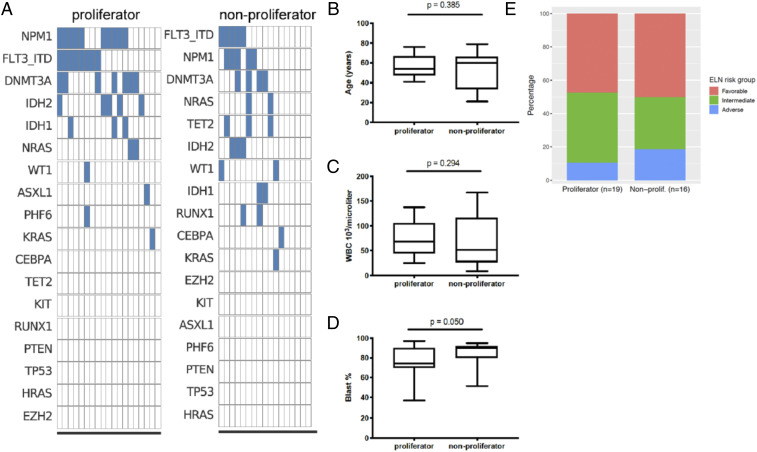
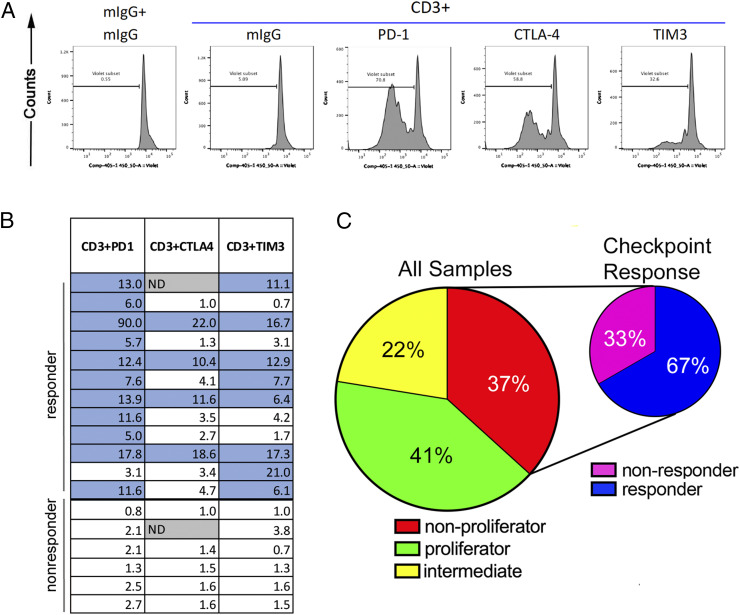
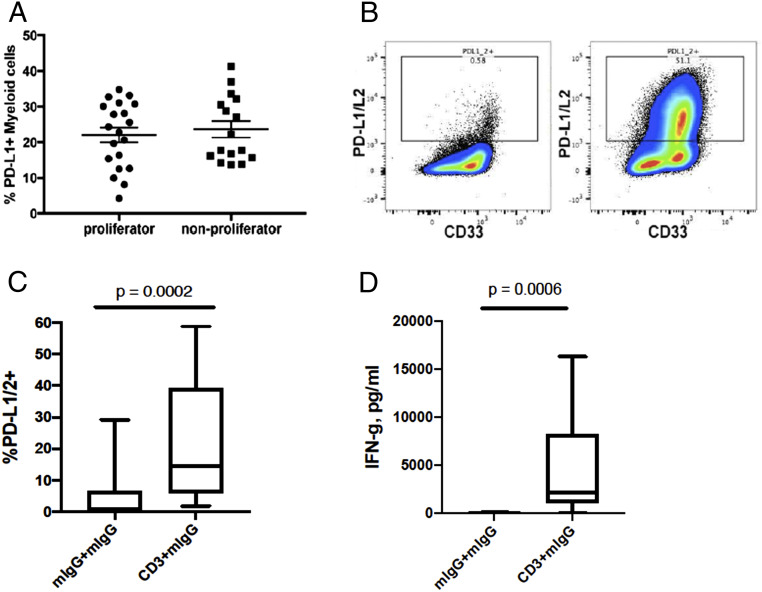
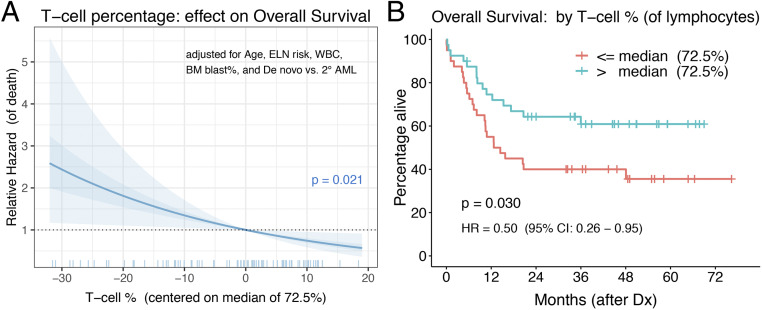
Acute myeloid leukemia (AML) is the most common acute leukemia in adults, with approximately four new cases per 100,000 persons per year. Standard treatment for AML consists of induction chemotherapy with remission achieved in 50 to 75% of cases. Unfortunately, most patients will relapse and die from their disease, as 5-y survival is roughly 29%. Therefore, other treatment options are urgently needed. In recent years, immune-based therapies have led to unprecedented rates of survival among patients with some advanced cancers. Suppression of T cell function in the tumor microenvironment is commonly observed and may play a role in AML. We found that there is a significant association between T cell infiltration in the bone marrow microenvironment of newly diagnosed patients with AML and increased overall survival. Functional studies aimed at establishing the degree of T cell suppression in patients with AML revealed impaired T cell function in many patients. In most cases, T cell proliferation could be restored by blocking the immune checkpoint molecules PD-1, CTLA-4, or TIM3. Our data demonstrate that AML establishes an immune suppressive environment in the bone marrow, in part through T cell checkpoint function.
Keywords: AML; T cell; checkpoint blockade; immune microenvironment; leukemia.
Copyright © 2020 the Author(s). Published by PNAS.
Conflict of interest statement
Competing interest statement: L.K.B., F.H., D.S., and H.A. are employees of Janssen Pharmaceuticals R&D, LLC. D.S. is currently an employee and holds stock in Genmab. C.V.L is an employee of Lab Connect LLC. J.N.S. receives research support form Kyn Therapeutics. B.J.D. has the following disclosures: Scientific Advisory Board for Aileron Therapeutics, ALLCRON, Cepheid, Vivid Biosciences, Celgene, RUNX1 Research Program, EnLiven Therapeutics, Gilead Sciences (inactive), Baxalta (inactive), Monojul (inactive); Scientific Advisory Board and Stock: Aptose Biosciences, Blueprint Medicines, Beta Cat, Iterion Therapeutics, Third Coast Therapeutics, GRAIL (inactive), CTI BioPharma (inactive); Scientific Founder: MolecularMD (inactive, acquired by ICON); Board of Directors and Stock: Amgen; Board of Directors: Burroughs Wellcome Fund, CureOne; Joint Steering Committee: Beat AML LLS; Founder: VB Therapeutics; Clinical Trial Funding: Novartis, Bristol-Myers Squibb, Pfizer; royalties from Patent 6958335 (Novartis exclusive license) and Oregon Health & Science University and Dana-Farber Cancer Institute (one Merck exclusive license). J.W.T. receives research support from Aptose, Array, AstraZeneca, Constellation, Genentech, Gilead, Incyte, Janssen, Petra, Seattle Genetics, Syros, and Takeda. J.W.T. is a cofounder of Leap Oncology. E.F.L. receives research support from Janssen Pharmaceuticals, Celgene Amgen, and Kyn Therapeutics.
Figures
References
-
- Deschler B., Lübbert M., Acute myeloid leukemia: Epidemiology and etiology. Cancer 107, 2099–2107 (2006). - PubMed
-
- National Cancer Institute Surveillance , Epidemiology, and End Results Program, Cancer Stat Facts: Leukemia — Acute Myeloid Leukemia (AML). https://seer.cancer.gov/statfacts/html/amyl.html. Accessed 26 May 2020.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
