

Morphological changes in intraretinal microvascular abnormalities after anti-VEGF therapy visualized on optical coherence tomography angiography
- PMID: 32514410
- PMCID: PMC7262762
- DOI: 10.1186/s40662-020-00195-2
Morphological changes in intraretinal microvascular abnormalities after anti-VEGF therapy visualized on optical coherence tomography angiography
Abstract
Background: To examine the baseline morphological characteristics and alterations in intraretinal microvascular abnormalities (IRMAs) in response to anti-vascular endothelial growth factor (anti-VEGF) treatment, documented by optical coherence tomography angiography (OCTA) in diabetic eyes.
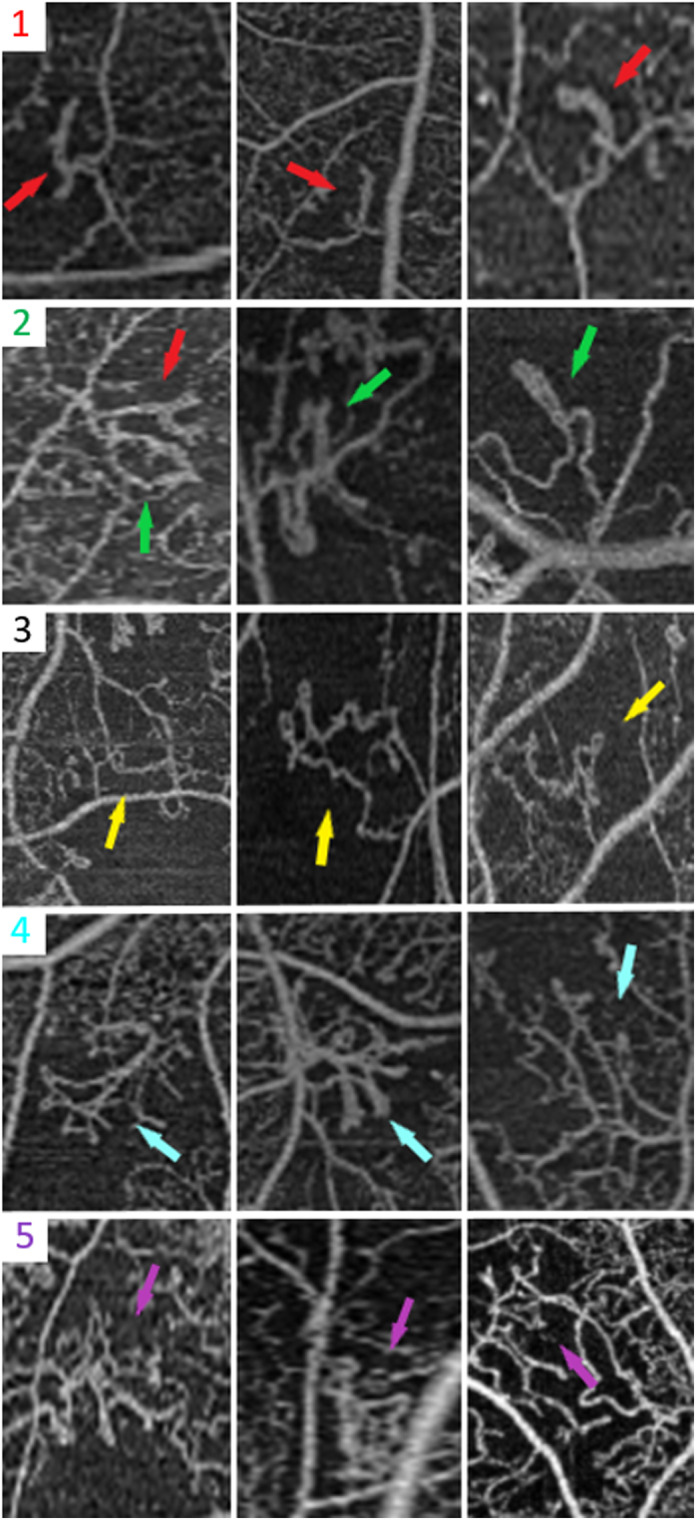
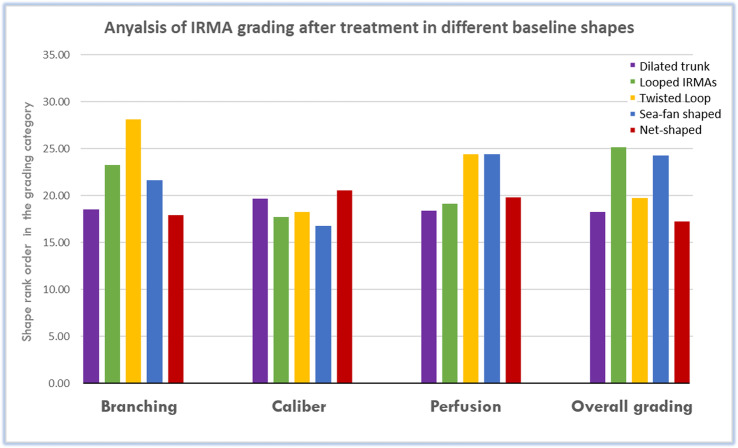
Methods: In this retrospective study, IRMAs were evaluated with multimodal imaging (fundus photography, fluorescein angiography, OCTA) in treatment-naïve diabetic eyes before and after anti-VEGF treatment for diabetic macular edema (DME) and/or proliferative diabetic retinopathy (PDR) and compared to diabetic control eyes with similar diabetic retinopathy (DR) severity that did not receive anti-VEGF therapy. The morphological characteristics of IRMAs on enface OCTA imaging were graded by masked readers at baseline, then after anti-VEGF therapy in treated eyes or after observation in control eyes. Characterization of interval changes in an IRMA were based on the following parameters: branching, vessel caliber and area of adjacent capillary non-perfusion.
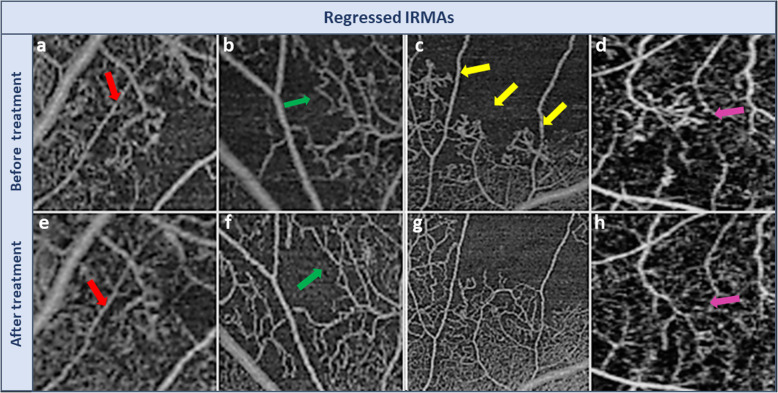
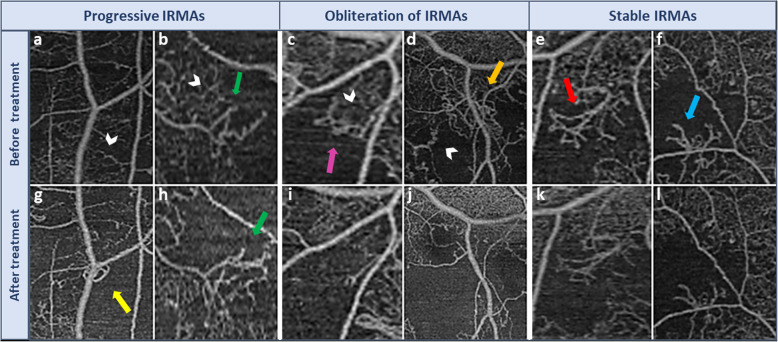
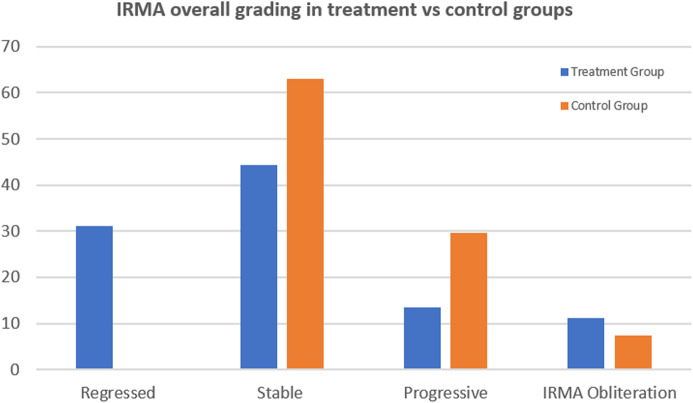
Results: The treated group included 45 IRMA foci from 15 eyes of 11 patients, while the control group included 27 IRMA foci from 15 eyes of 14 patients. Following anti-VEGF treatment, enface OCTA demonstrated that 14 foci of IRMA (31%) demonstrated regression with normalization of appearance of the capillary bed, 20 IRMAs (44%) remained unchanged, six IRMAs (13%) progressed with enlargement or development of new IRMAs and five IRMAs (11%) demonstrated complete obliteration defined as IRMA disappearance with advancing capillary drop-out. In the control group, 17 IRMA (63%) remained stable, 8 IRMAs (29.6%) progressed and 2 experienced total obliteration (7.4%). The difference in rank order between the two groups was statistically significant (p = 0.022).
Conclusions: In eyes with DR status post anti-VEGF therapy, foci of IRMAs have a variable course demonstrating one of four possible outcomes: regression, stability, progression or complete obliteration. In contrast, none of the untreated control diabetic eyes demonstrated regression of IRMAs, consistent with known progression of DR severity in high risk eyes. Morphologic evaluation of IRMAs with OCTA may help to monitor changes in retinal blood flow as well as the response to anti-VEGF treatment.
Keywords: Anti-VEGF; DME; Ischemia; OCTA; PDR; Retina.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests relevant to this study, and their detailed financial disclosure: OS: None; NM: None; CB: Consultant, Genentech, Speaker, Carl Zeiss Meditec, Novartis; AI: Speaker, Topcon Medical Systems, Inc., Nidek Medical Products, Inc.; KL: None; EK: none; SM: None; A.YA: None; MA: None; AW: None; JD: Consultant and Financial Support, Carl Zeiss Meditec, Inc., Optovue, Inc., Novartis Pharma AG., and Roche; NW: Financial Support, Macula Vision Research Foundation, Topcon Medical Systems, Inc., Nidek Medical Products, Inc., and Carl Zeiss Meditec, Inc., Consultant, Optovue, Inc., Regeneron, and Genentech.
Figures
References
-
- Early Treatment Diabetic Retinopathy Study Research Group Grading diabetic retinopathy from stereoscopic color fundus photographs--an extension of the modified Airlie House classification. ETDRS report number 10. Ophthalmology. 1991;98(5 Suppl):786–806. - PubMed
-
- Early Treatment Diabetic Retinopathy Study design and baseline patient characteristics. ETDRS report number 7. Ophthalmology. 1991;98(5 Suppl):741–56. - PubMed
-
- Writing Committee for the Diabetic Retinopathy Clinical Research Network. Gross JG, Glassman AR, Jampol LM, Inusah S, Aiello LP, Antoszyk AN, et al. Panretinal photocoagulation vs intravitreous ranibizumab for proliferative diabetic retinopathy: a randomized clinical trial. JAMA. 2015;314(20):2137–2146. doi: 10.1001/jama.2015.15217. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
