

Genetic Mouse Models and Induced Pluripotent Stem Cells for Studying Tracheal-Esophageal Separation and Esophageal Development
- PMID: 32515280
- PMCID: PMC9839344
- DOI: 10.1089/scd.2020.0075
Genetic Mouse Models and Induced Pluripotent Stem Cells for Studying Tracheal-Esophageal Separation and Esophageal Development
Abstract
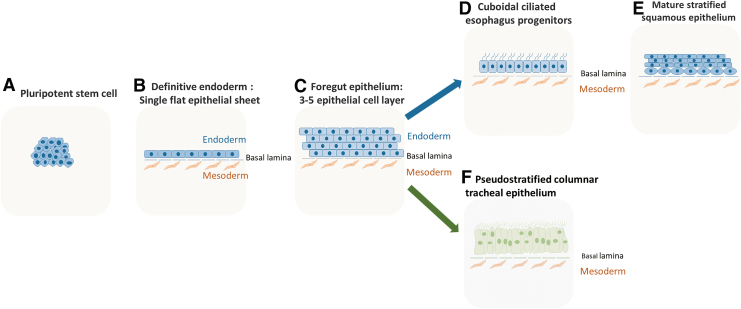
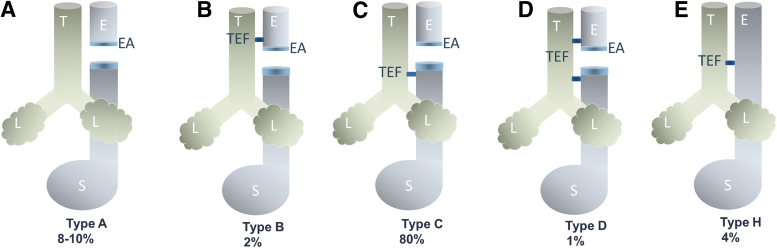
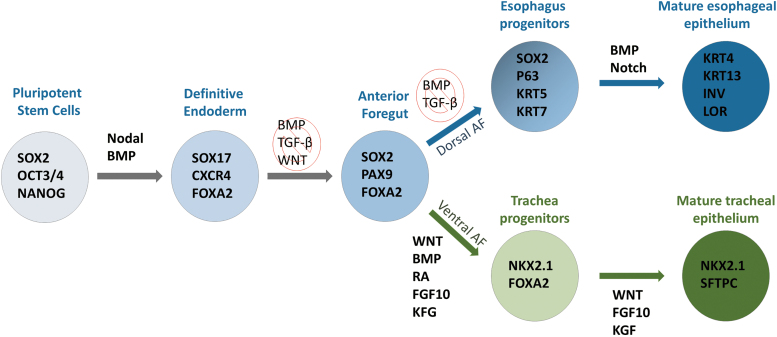
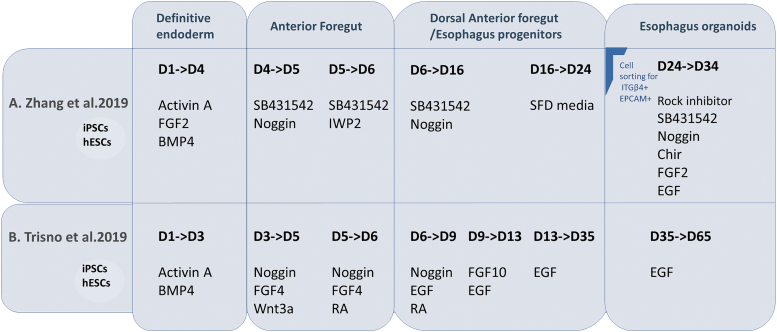
Esophagus and trachea arise from a common origin, the anterior foregut tube. The compartmentalization process of the foregut into the esophagus and trachea is still poorly understood. Esophageal atresia/tracheoesophageal fistula (EA/TEF) is one of the most common gastrointestinal congenital defects with an incidence rate of 1 in 2,500 births. EA/TEF is linked to the disruption of the compartmentalization process of the foregut tube. In EA/TEF patients, other organ anomalies and disorders have also been reported. Over the last two decades, animal models have shown the involvement of multiple signaling pathways and transcription factors in the development of the esophagus and trachea. Use of induced pluripotent stem cells (iPSCs) to understand organogenesis has been a valuable tool for mimicking gastrointestinal and respiratory organs. This review focuses on the signaling mechanisms involved in esophageal development and the use of iPSCs to model and understand it.
Keywords: esophageal atresia/tracheoesophageal fistula; esophageal organoids; induced pluripotent stem cells.
Conflict of interest statement
No competing financial interests exist.
Figures


Similar articles
-
iPSCs derived from esophageal atresia patients reveal SOX2 dysregulation at the anterior foregut stage.Dis Model Mech. 2022 Nov 1;15(11):dmm049541. doi: 10.1242/dmm.049541. Epub 2022 Nov 28. Dis Model Mech. 2022. PMID: 36317486 Free PMC article.
-
Compartmentalization of the foregut tube: developmental origins of the trachea and esophagus.Wiley Interdiscip Rev Dev Biol. 2012 Mar-Apr;1(2):184-202. doi: 10.1002/wdev.12. Epub 2011 Nov 21. Wiley Interdiscip Rev Dev Biol. 2012. PMID: 23801435 Review.
-
One shall become two: Separation of the esophagus and trachea from the common foregut tube.Dev Dyn. 2015 Mar;244(3):277-88. doi: 10.1002/dvdy.24219. Epub 2014 Dec 2. Dev Dyn. 2015. PMID: 25329576 Free PMC article. Review.
-
BMP antagonism by Noggin is required in presumptive notochord cells for mammalian foregut morphogenesis.Dev Biol. 2014 Jul 1;391(1):111-24. doi: 10.1016/j.ydbio.2014.02.008. Epub 2014 Mar 12. Dev Biol. 2014. PMID: 24631216
-
Developmental basis of trachea-esophageal birth defects.Dev Biol. 2021 Sep;477:85-97. doi: 10.1016/j.ydbio.2021.05.015. Epub 2021 May 21. Dev Biol. 2021. PMID: 34023332 Free PMC article. Review.
Cited by
-
Delayed primary anastomosis for repair of long-gap esophageal atresia: technique revisited.Pediatr Surg Int. 2022 Dec 8;39(1):40. doi: 10.1007/s00383-022-05317-6. Pediatr Surg Int. 2022. PMID: 36482208 Free PMC article.
-
Patient-derived tumor models: a suitable tool for preclinical studies on esophageal cancer.Cancer Gene Ther. 2023 Nov;30(11):1443-1455. doi: 10.1038/s41417-023-00652-9. Epub 2023 Aug 3. Cancer Gene Ther. 2023. PMID: 37537209 Review.
-
iPSCs derived from esophageal atresia patients reveal SOX2 dysregulation at the anterior foregut stage.Dis Model Mech. 2022 Nov 1;15(11):dmm049541. doi: 10.1242/dmm.049541. Epub 2022 Nov 28. Dis Model Mech. 2022. PMID: 36317486 Free PMC article.
-
Generation of three induced pluripotent stem cells lines from patients with esophageal atresia/tracheoesophageal fistula type C.Stem Cell Res. 2022 Apr;60:102711. doi: 10.1016/j.scr.2022.102711. Epub 2022 Feb 18. Stem Cell Res. 2022. PMID: 35193008 Free PMC article.
-
Directed differentiation of human embryonic stem cells into parathyroid cells and establishment of parathyroid organoids.Cell Prolif. 2024 Aug;57(8):e13634. doi: 10.1111/cpr.13634. Epub 2024 Mar 18. Cell Prolif. 2024. PMID: 38494923 Free PMC article.
References
-
- Yu WY, Slack JM and Tosh D. (2005). Conversion of columnar to stratified squamous epithelium in the developing mouse oesophagus. Dev Biol 284:157–170. - PubMed
-
- van Lennep M, Singendonk MMJ, Dall'Oglio L, Gottrand F, Krishnan U, Terheggen-Lagro SWJ, Omari TI, Benninga MA and van Wijk MP. (2019). Oesophageal atresia. Nat Rev Dis Primers 5:26. - PubMed
-
- Peters JH and Avisar N. (2010). The molecular pathogenesis of Barrett's esophagus: common signaling pathways in embryogenesis metaplasia and neoplasia. J Gastrointest Surg 14(Suppl. 1):S81–S87. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
