

Identifying scenarios of benefit or harm from kidney transplantation during the COVID-19 pandemic: A stochastic simulation and machine learning study
- PMID: 32515544
- PMCID: PMC7300693
- DOI: 10.1111/ajt.16117
Identifying scenarios of benefit or harm from kidney transplantation during the COVID-19 pandemic: A stochastic simulation and machine learning study
Abstract
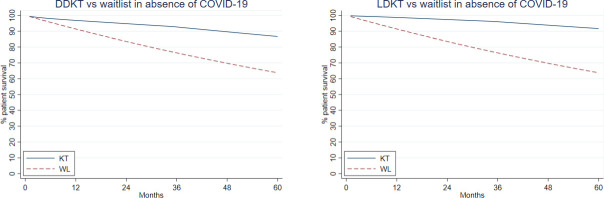
Clinical decision-making in kidney transplant (KT) during the coronavirus disease 2019 (COVID-19) pandemic is understandably a conundrum: both candidates and recipients may face increased acquisition risks and case fatality rates (CFRs). Given our poor understanding of these risks, many centers have paused or reduced KT activity, yet data to inform such decisions are lacking. To quantify the benefit/harm of KT in this context, we conducted a simulation study of immediate-KT vs delay-until-after-pandemic for different patient phenotypes under a variety of potential COVID-19 scenarios. A calculator was implemented (http://www.transplantmodels.com/covid_sim), and machine learning approaches were used to evaluate the important aspects of our modeling. Characteristics of the pandemic (acquisition risk, CFR) and length of delay (length of pandemic, waitlist priority when modeling deceased donor KT) had greatest influence on benefit/harm. In most scenarios of COVID-19 dynamics and patient characteristics, immediate KT provided survival benefit; KT only began showing evidence of harm in scenarios where CFRs were substantially higher for KT recipients (eg, ≥50% fatality) than for waitlist registrants. Our simulations suggest that KT could be beneficial in many centers if local resources allow, and our calculator can help identify patients who would benefit most. Furthermore, as the pandemic evolves, our calculator can update these predictions.
Keywords: Scientific Registry for Transplant Recipients (SRTR); clinical research/practice; infection and infectious agents; kidney transplantation/nephrology.
© 2020 The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures




Comment in
-
Kidney transplant in the COVID era: Cautious optimism and continued vigilance.Am J Transplant. 2020 Nov;20(11):2971-2972. doi: 10.1111/ajt.16190. Epub 2020 Jul 28. Am J Transplant. 2020. PMID: 32654275 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
