

doi: 10.1164/rccm.202005-1586LE.
Ventilator Sharing during an Acute Shortage Caused by the COVID-19 Pandemic
Affiliations
- PMID: 32515988
- PMCID: PMC7427377
- DOI: 10.1164/rccm.202005-1586LE
Item in Clipboard
Ventilator Sharing during an Acute Shortage Caused by the COVID-19 Pandemic
Am J Respir Crit Care Med.
.
No abstract available
Figures
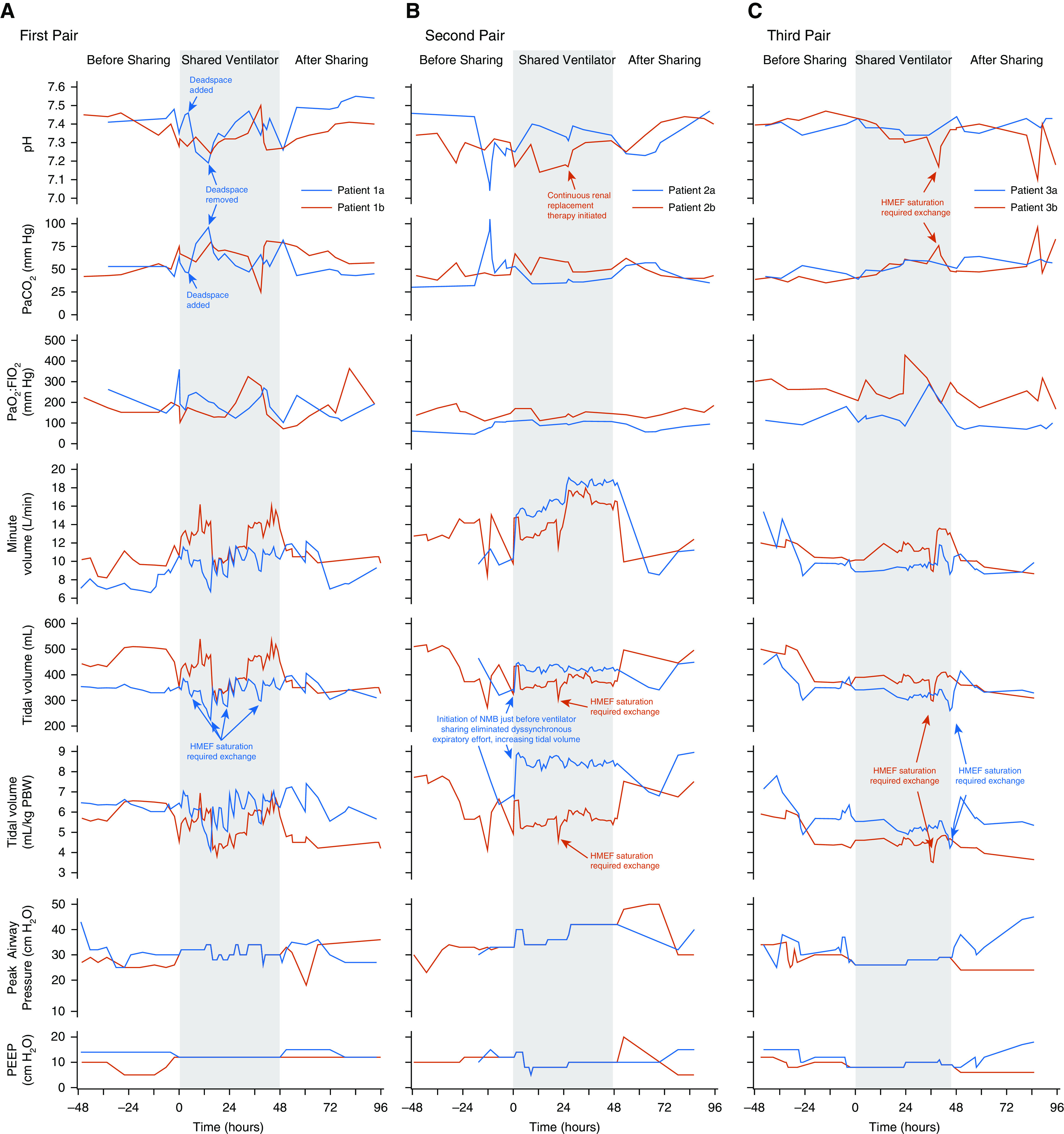
Clinical course of patients during ventilator sharing and for 48 hours preceding and afterward. (A) First pair. Patients shared a repurposed anesthesia machine. Approximately 4.5 hours after initiating ventilator sharing, patient 1a became alkalemic (pH 7.46), whereas patient 1b remained acidemic (pH 7.28). To treat alkalemia, deadspace tubing was added to the circuit of patient 1a, but resulting pH was lower than intended; with removal of this deadspace tubing, acidemia promptly improved. The HMEF had to be changed frequently for both patient circuits as CO2 absorbent-related moisture buildup increased resistance, an effect most pronounced in patient 1a. (B) Second pair. Patients shared a full-feature ICU ventilator. Patient 2a’s course illustrated the importance of ensuring steady-state ventilator requirements and reconfirming compatibility on neuromuscular blockade before initiating sharing. Patient 2a was intubated for 16 hours prior to ventilator sharing. During compatibility assessment, ventilator settings were matched and well tolerated but compatibility not reconfirmed after starting neuromuscular blockade in patient 2a; the patient exhibited overt, dyssynchronous expiratory effort before paralysis, and eliminating respiratory muscle activity substantially increased Vt for a given driving pressure. Patient 2b was initiated on renal replacement therapy at Hour 28 for renal failure, which promptly increased pH. The patient’s renal failure and plan for renal replacement predated ventilator sharing. (C) Third pair. Patients shared a full-feature ICU ventilator. Vt and acid–base balance were well controlled during ventilator sharing, reflecting cumulative experience and protocol refinement with incorporation of lessons learned. Patient 3b experienced a transient decrease in Vt and pH and increase in PaCO2 around Hour 36 owing to HMEF oversaturation that promptly resolved with its exchange. HMEF = heat and moisture exchanging filter; NMB = neuromuscular blockade; PBW = predicted body weight; PEEP = positive end-expiratory pressure.
Comment in
-
Ventilator Sharing during Shortages. A Siren's Song?Am J Respir Crit Care Med. 2020 Aug 15;202(4):490-491. doi: 10.1164/rccm.202006-2438ED. Am J Respir Crit Care Med. 2020. PMID: 32610021 Free PMC article. No abstract available.
-
In-Parallel Ventilator Sharing during an Acute Shortage: Too Much Risk for a Wider Uptake.Am J Respir Crit Care Med. 2020 Nov 1;202(9):1316-1317. doi: 10.1164/rccm.202006-2420LE. Am J Respir Crit Care Med. 2020. PMID: 32744454 Free PMC article. No abstract available.
-
Ventilator Sharing Using Volume-controlled Ventilation during the COVID-19 Pandemic.Am J Respir Crit Care Med. 2020 Nov 1;202(9):1317-1319. doi: 10.1164/rccm.202006-2452LE. Am J Respir Crit Care Med. 2020. PMID: 32744456 Free PMC article. No abstract available.
-
Reply to Chase et al. and to Milner et al.Am J Respir Crit Care Med. 2020 Nov 1;202(9):1319-1320. doi: 10.1164/rccm.202007-2959LE. Am J Respir Crit Care Med. 2020. PMID: 32744458 Free PMC article. No abstract available.
References
-
- Feuer A, Rosenthal BM.Coronavirus in N.Y.: ‘astronomical’ surge leads to quarantine warning New York Times 2020 [created 2020 Mar 24; accessed 2020 Mar 24]. Available from: https://www.nytimes.com/2020/03/24/nyregion/coronavirus-new-york-apex-an...
-
- Cuomo A.New York State governor’s daily coronavirus press briefing 2020[created 2020 Mar 29; accessed 2020 Mar 29]. Available from: https://www.governor.ny.gov/news/amid-ongoing-covid-19-pandemic-governor...
-
- Amato MBP, Meade MO, Slutsky AS, Brochard L, Costa ELV, Schoenfeld DA, et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. 2015;372:747–755. - PubMed
-
- Branson RD, Blakeman TC, Robinson BR, Johannigman JA. Use of a single ventilator to support 4 patients: laboratory evaluation of a limited concept. Respir Care. 2012;57:399–403. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
