

Predicting the Pathologic Complete Response After Neoadjuvant Pembrolizumab in Muscle-Invasive Bladder Cancer
- PMID: 32516377
- PMCID: PMC7781448
- DOI: 10.1093/jnci/djaa076
Predicting the Pathologic Complete Response After Neoadjuvant Pembrolizumab in Muscle-Invasive Bladder Cancer
Abstract
Background: In the PURE-01 study (NCT02736266), we aimed to evaluate the ability to predict the pathologic complete response (pT0N0) after pembrolizumab by using clinical and tumor biomarkers.
Methods: In an open-label, single-arm, phase 2 study, 3 courses of 200 mg pembrolizumab preceding radical cystectomy were administered in patients with T2-4aN0M0 muscle-invasive bladder cancer. The analyses included a comprehensive genomic profiling and programmed cell-death-ligand-1 (PD-L1)-combined positive score assessment (CPS; Dako 22C3 antibody) of pre- and posttherapy samples. Multivariable logistic regression analyses evaluated baseline clinical T stage and tumor biomarkers in association with pT0N0 response. Corresponding coefficients were used to develop a calculator of pT0N0 response based on the tumor mutational burden (TMB), CPS, and the clinical T stage. Decision-curve analysis was also performed. All statistical tests were 2-sided.
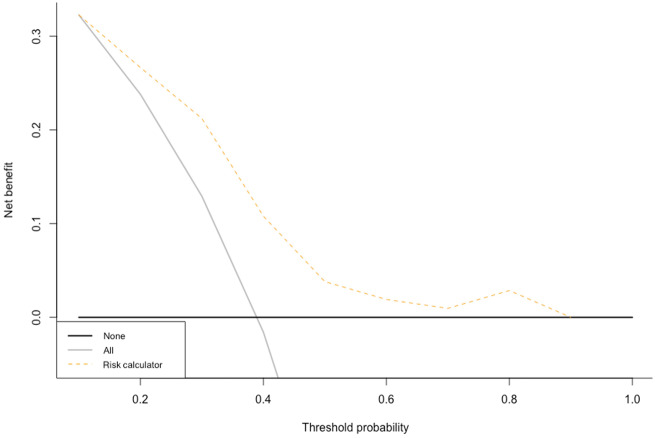
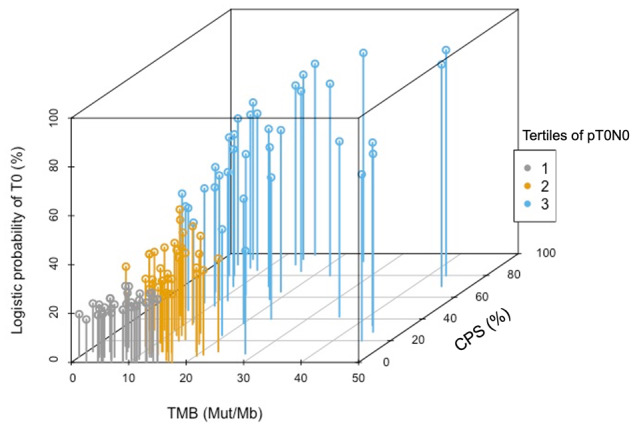
Results: From February 2017 to June 2019, 112 patients with biomarker data were enrolled (105 with complete TMB and CPS data). Increasing TMB and CPS values featured a linear association with logistic pT0N0 probabilities (P = .02 and P = .004, respectively). For low TMB values (≤11 mut/Mb, median value, n = 53), pT0N0 probability was not associated with increasing CPS. Conversely, for high TMB values (>11 mut/Mb, n = 52), pT0N0 was statistically significantly associated with higher CPS (P = .004). The C index of the pT0N0 probability calculator was 0.77. On decision-curve analysis, the net benefit of the model was higher than the "treat-all" option within the clinically meaningful threshold probabilities of 40%-50%.
Conclusions: The study presents a composite biomarker-based pT0N0 probability calculator that reveals the complex interplay between TMB and CPS, added to the clinical T stage.
© The Author(s) 2020. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Multifactorial, Biomarker-Based Predictive Models for Immunotherapy Response Enter the Arena.J Natl Cancer Inst. 2021 Jan 4;113(1):7-8. doi: 10.1093/jnci/djaa077. J Natl Cancer Inst. 2021. PMID: 32516413 Free PMC article. No abstract available.
-
Urological Oncology: Bladder, Penis and Urethral Cancer, and Basic Principles of Oncology.J Urol. 2022 May;207(5):1153-1155. doi: 10.1097/JU.0000000000002460. Epub 2022 Feb 10. J Urol. 2022. PMID: 35139651 No abstract available.
References
-
- Alfred Witjes J, Lebret T, Compérat EM, et al.Updated 2016 EAU guidelines on muscle-invasive and metastatic bladder cancer. Eur Urol. 2017;71(3):462–475. - PubMed
-
- Witjies JA, Bruins M, Cathomas R, et al. EAU Guidelines. Edn. Presented at the EAU Annual Congress Barcelona; 2019. ISBN 978-94-92671-04-2.
-
- Grossman HB, Natale RB, Tangen CM, et al.Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003;349(9):859–866. - PubMed
-
- Niglio SA, Jia R, Ji J, et al.Programmed death-1 or programmed death ligand-1 blockade in patients with platinum-resistant metastatic urothelial cancer: a systematic review and meta-analysis. Eur Urol. 2019;76:782–789. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
