

Risk factors for transplant-associated thrombotic microangiopathy and mortality in a pediatric cohort
- PMID: 32516415
- PMCID: PMC7284101
- DOI: 10.1182/bloodadvances.2019001242
Risk factors for transplant-associated thrombotic microangiopathy and mortality in a pediatric cohort
Abstract
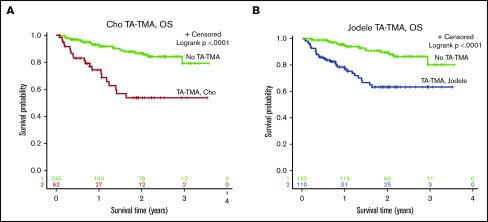
Transplant-associated thrombotic microangiopathy (TA-TMA) is a well-recognized complication of hematopoietic cell transplantation (HCT). Diagnosis is challenging and in the absence of a tissue biopsy, TA-TMA is provisionally diagnosed by meeting clinical criteria. In this study, we describe the prevalence, outcomes, and risk factors for meeting 2 different diagnostic criteria for TA-TMA and for increased transplant-related mortality (TRM). In this retrospective study of 307 pediatric HCT patients, records were reviewed for the first 100 days after HCT. Patients who were diagnosed with TA-TMA by a provider during this time were included. In addition, the Cho et al criteria (2010) and Jodele et al (2014) TA-TMA criteria were applied retrospectively. Eight patients (2.6%) were diagnosed with TA-TMA by their provider. However, on retrospective review, 20% and 36% met the Cho and Jodele criteria for TA-TMA, respectively. Overall survival was significantly worse (P < .0001) and TRM was significantly higher in patients who met criteria for TA-TMA (MC-TA-TMA) (P < .0001). After controlling for comorbid conditions, MC-TA-TMA (hazard ratio [HR], 10.9; P = .0001) and grade 3/4 acute graft-versus-host-disease (aGVHD) (HR 3.5; P = .01) remained independently associated with increased TRM. Among allogeneic HCT recipients, features associated with an increased risk for MC-TA-TMA included ≥2 HCT, concurrent grade 3/4 aGVHD and concurrent infections. Among patients who MC-TA-TMA, LDH ≥2 times the upper limit of normal (P = .001), the need for ≥2 antihypertensive medications (P < .0001), and acute kidney injury (P = .003) were associated with significantly increased TRM.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures




References
-
- Labrador J, López-Corral L, López-Godino O, et al. . Risk factors for thrombotic microangiopathy in allogeneic hematopoietic stem cell recipients receiving GVHD prophylaxis with tacrolimus plus MTX or sirolimus. Bone Marrow Transplant. 2014;49(5):684-690. - PubMed
-
- Jodele S, Dandoy C, Myers K, et al. . High-dose carboplatin/etoposide/melphalan increases risk of thrombotic microangiopathy and organ injury after autologous stem cell transplantation in patients with neuroblastoma. Bone Marrow Transplant. 2018;53(10):1311-1318. - PubMed
-
- Ho V, Cutler C, Carter S, et al. . Blood and marrow transplant clinical trials network toxicity committee consensus summary: thrombotic microangiopathy after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2005;11(8):571-575. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
