

Performance of the GRACE 2.0 score in patients with type 1 and type 2 myocardial infarction
- PMID: 32516805
- PMCID: PMC8266602
- DOI: 10.1093/eurheartj/ehaa375
Performance of the GRACE 2.0 score in patients with type 1 and type 2 myocardial infarction
Abstract
Aims: The Global Registry of Acute Coronary Events (GRACE) score was developed to evaluate risk in patients with myocardial infarction. However, its performance in type 2 myocardial infarction is uncertain.
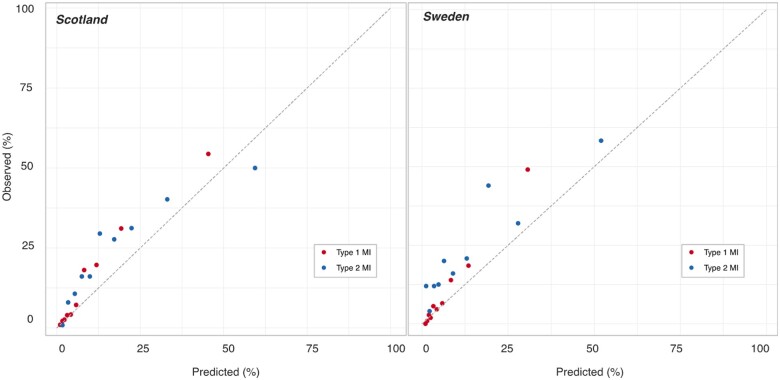
Methods and results: In two cohorts of consecutive patients with suspected acute coronary syndrome from 10 hospitals in Scotland (n = 48 282) and a tertiary care hospital in Sweden (n = 22 589), we calculated the GRACE 2.0 score to estimate death at 1 year. Discrimination was evaluated by the area under the receiver operating curve (AUC), and compared for those with an adjudicated diagnosis of type 1 and type 2 myocardial infarction using DeLong's test. Type 1 myocardial infarction was diagnosed in 4981 (10%) and 1080 (5%) patients in Scotland and Sweden, respectively. At 1 year, 720 (15%) and 112 (10%) patients died with an AUC for the GRACE 2.0 score of 0.83 [95% confidence interval (CI) 0.82-0.85] and 0.85 (95% CI 0.81-0.89). Type 2 myocardial infarction occurred in 1121 (2%) and 247 (1%) patients in Scotland and Sweden, respectively, with 258 (23%) and 57 (23%) deaths at 1 year. The AUC was 0.73 (95% CI 0.70-0.77) and 0.73 (95% CI 0.66-0.81) in type 2 myocardial infarction, which was lower than for type 1 myocardial infarction in both cohorts (P < 0.001 and P = 0.008, respectively).
Conclusion: The GRACE 2.0 score provided good discrimination for all-cause death at 1 year in patients with type 1 myocardial infarction, and moderate discrimination for those with type 2 myocardial infarction.
Trial registration: ClinicalTrials.gov number, NCT01852123.
Keywords: GRACE; High-sensitivity; Troponin; Type 1 myocardial infarction; Type 2 myocardial infarction; Universal definition.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures



Comment in
-
Has the Fourth Universal Definition of Myocardial Infarction led to better diagnosis and risk stratification?Eur Heart J. 2021 Jul 8;42(26):2562-2564. doi: 10.1093/eurheartj/ehaa486. Eur Heart J. 2021. PMID: 32647857 No abstract available.
References
-
- Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J 2016;37:3232–3245. - PubMed
-
- Eagle KA, Lim MJ, Dabbous OH, Pieper KS, Goldberg RJ, Van de Werf F, Goodman SG, Granger CB, Steg PG, Gore JM, Budaj A, Avezum A, Flather MD, Fox KA; GRACE Investigators. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month post discharge death in an international registry. JAMA 2004;291:2727–2733. - PubMed
-
- Fox KA, Dabbous OH, Goldberg RJ, Pieper KS, Eagle KA, Van de Werf F, Avezum A, Goodman SG, Flather MD, Anderson FA Jr, Granger CB. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE). BMJ 2006;333:1091. - PMC - PubMed
-
- Fox KA, Fitzgerald G, Puymirat E, Huang W, Carruthers K, Simon T, Coste P, Monsegu J, Steg GS, Danchin N, Anderson F. Should patients with acute coronary disease be stratified for management according to their risk? Derivation, external validation and outcomes using the updated GRACE risk score. BMJ Open 2014;4:e004425. - PMC - PubMed
-
- Granger CB, Goldberg RJ, Dabbous O, Pieper KS, Eagle KA, Cannon CP, Van D, Werf F, Avezum A, Goodman SG, Flather MD, Fox KA, Grace I. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med 2003;163:2345–2353. - PubMed
