

Significance and Diagnostic Accuracy of Early S100B Serum Concentration after Aneurysmal Subarachnoid Hemorrhage
- PMID: 32516898
- PMCID: PMC7356310
- DOI: 10.3390/jcm9061746
Significance and Diagnostic Accuracy of Early S100B Serum Concentration after Aneurysmal Subarachnoid Hemorrhage
Abstract
Background: Early brain injuries (EBI) are one of the most important causes of morbidity and mortality after subarachnoid hemorrhage. At admission, a third of patients are unconscious (spontaneously or sedated) and EBI consequences are not evaluable. To date, it is unclear who will still be comatose (with severe EBI) and who will recover (with less severe EBI) once the aneurysm is treated and sedation withdrawn. The objective of the present study was to determine the diagnostic accuracy of S100B levels at hospital admission to identify patients with severe neurological consequences of EBI.
Methods: Patients were consecutively included in this prospective blinded observational study. A motor component of the Glasgow coma score under 6 on day 3 was used to define patients with severe neurological consequences of EBI.
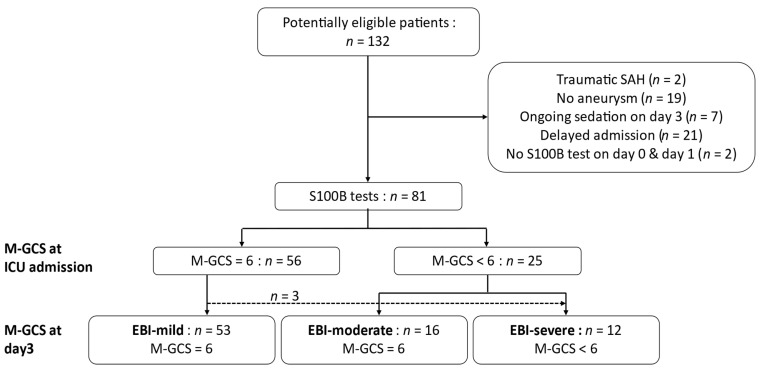
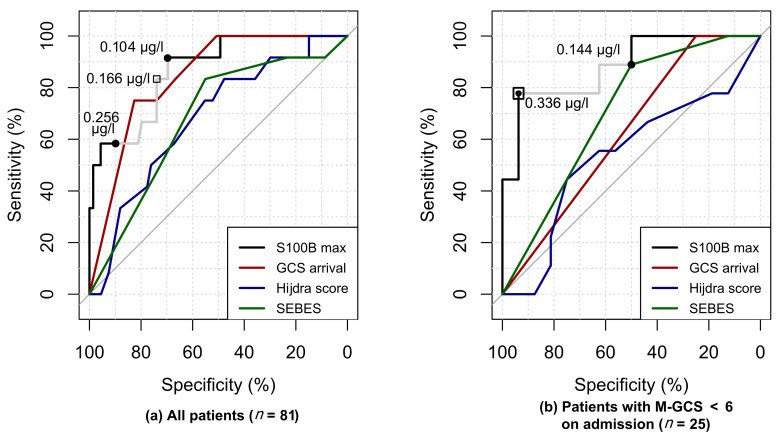
Results: A total of 81 patients were included: 25 patients were unconscious at admission, 68 were treated by coiling. On day 3, 12 patients had severe consequences of EBI. A maximal S100B value between admission and day 1 had an area under the receiver operating characteristic curve (AUC) of 86.7% to predict severe EBI consequences. In patients with impaired consciousness at admission, the AUC was 88.2%.
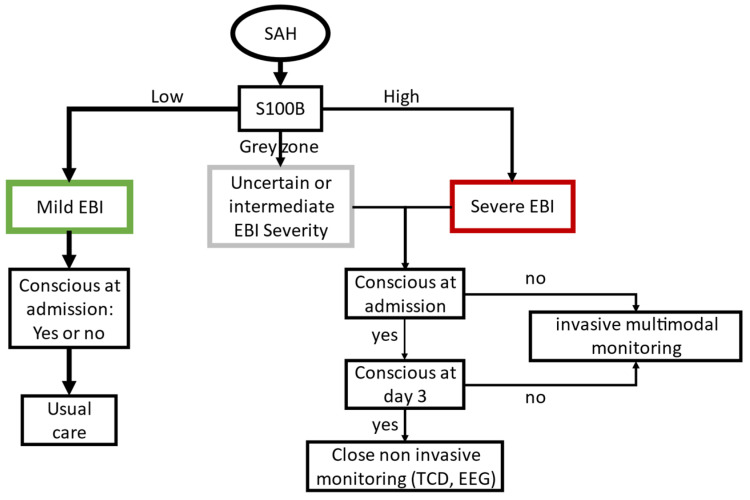
Conclusion: Early S100B seems to have a good diagnostic value to predict severe EBI. Before claiming the usefulness of S100B as a surrogate marker of EBI severity to start earlier multimodal monitoring, these results must be confirmed in an independent validation cohort.
Keywords: S100B protein; early brain injury; patient outcome assessment; subarachnoid hemorrhage.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Connolly S.E., Rabinstein A.A., Carhuapoma R.J., Derdeyn C.P., Dion J., Higashida R.T., Hoh B.L., Kirkness C.J., Naidech A.M., Ogilvy C.S., et al. Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2012;43:1711–1737. doi: 10.1161/STR.0b013e3182587839. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
