

Prevalence and Impact of Myocardial Injury in Patients Hospitalized With COVID-19 Infection
- PMID: 32517963
- PMCID: PMC7279721
- DOI: 10.1016/j.jacc.2020.06.007
Prevalence and Impact of Myocardial Injury in Patients Hospitalized With COVID-19 Infection
Abstract
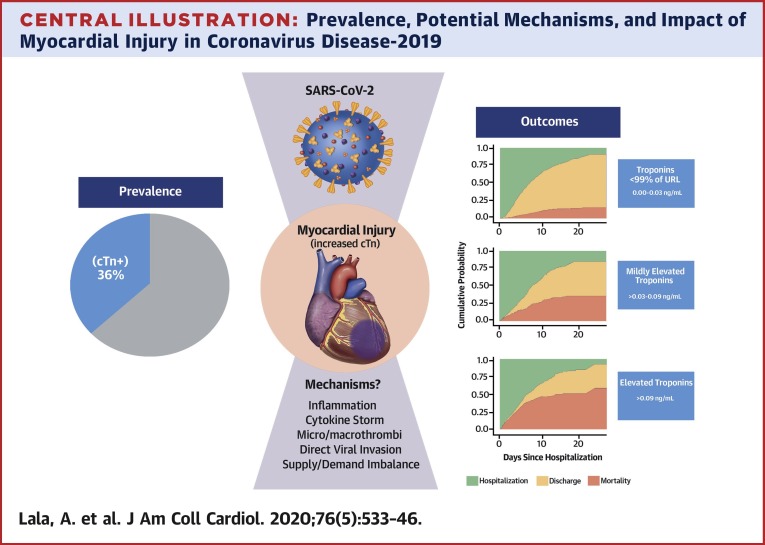
Background: The degree of myocardial injury, as reflected by troponin elevation, and associated outcomes among U.S. hospitalized patients with coronavirus disease-2019 (COVID-19) are unknown.
Objectives: The purpose of this study was to describe the degree of myocardial injury and associated outcomes in a large hospitalized cohort with laboratory-confirmed COVID-19.
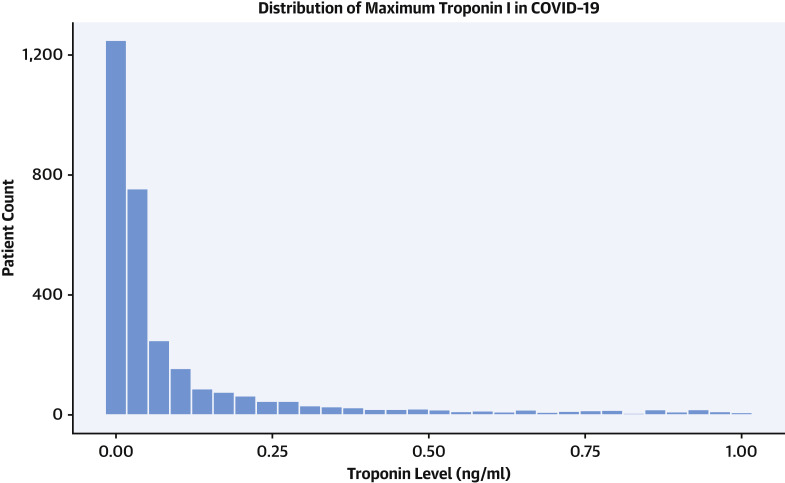
Methods: Patients with COVID-19 admitted to 1 of 5 Mount Sinai Health System hospitals in New York City between February 27, 2020, and April 12, 2020, with troponin-I (normal value <0.03 ng/ml) measured within 24 h of admission were included (n = 2,736). Demographics, medical histories, admission laboratory results, and outcomes were captured from the hospitals' electronic health records.
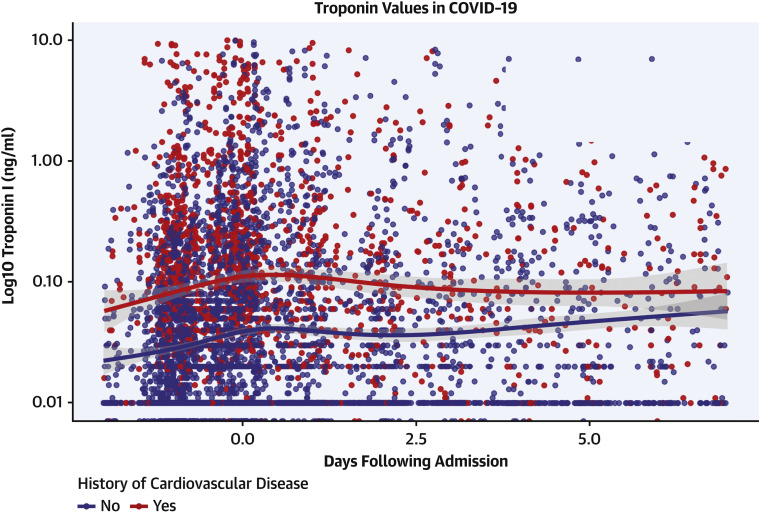
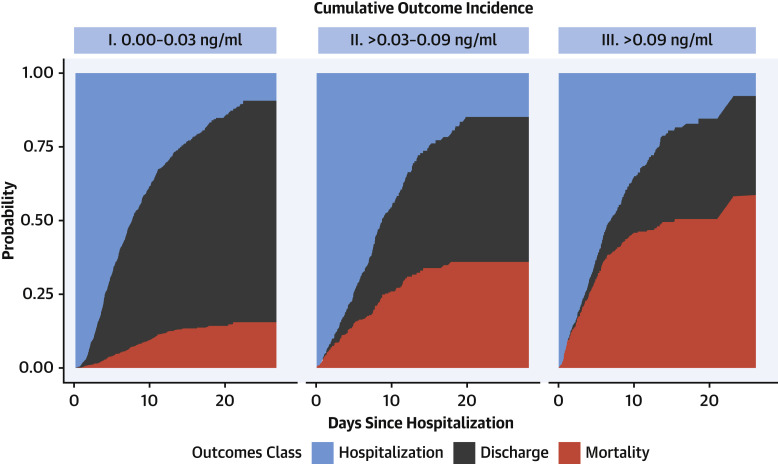
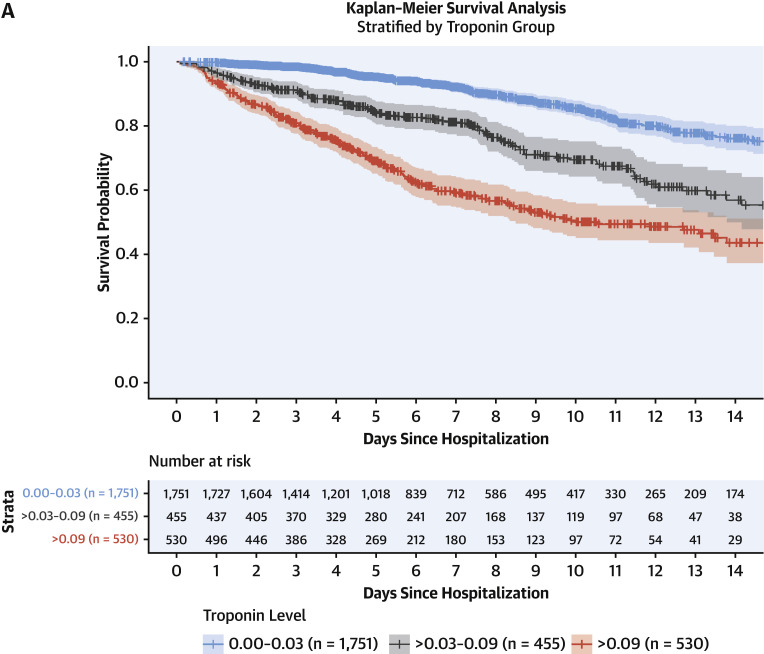
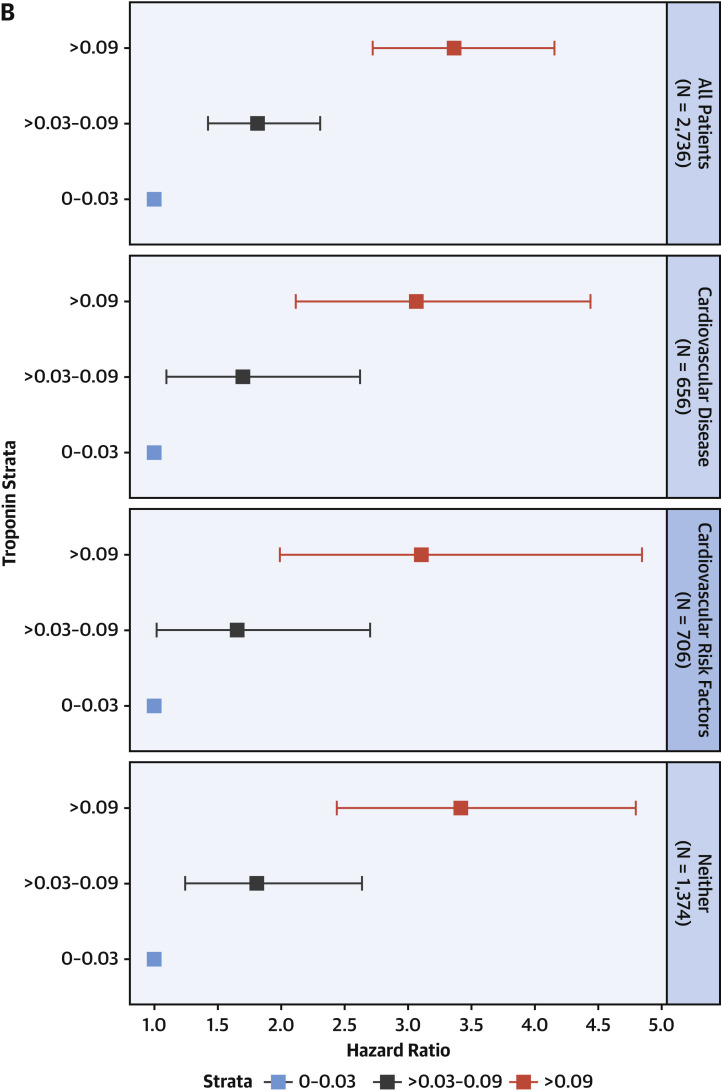
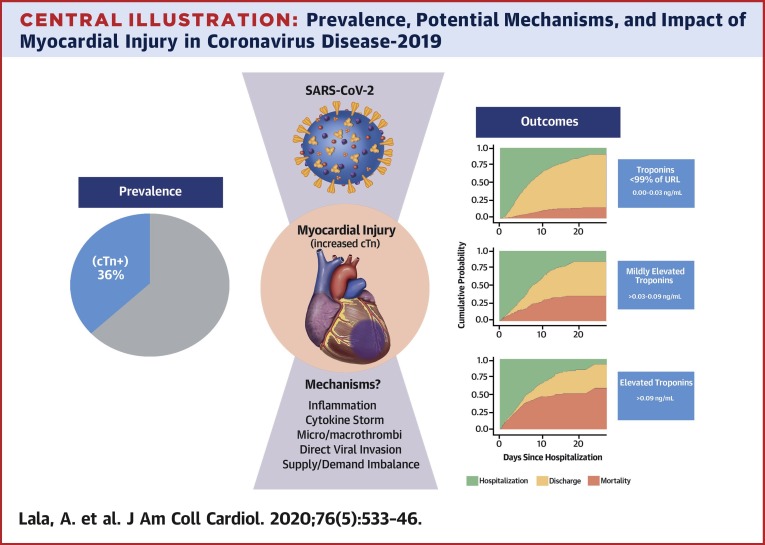
Results: The median age was 66.4 years, with 59.6% men. Cardiovascular disease (CVD), including coronary artery disease, atrial fibrillation, and heart failure, was more prevalent in patients with higher troponin concentrations, as were hypertension and diabetes. A total of 506 (18.5%) patients died during hospitalization. In all, 985 (36%) patients had elevated troponin concentrations. After adjusting for disease severity and relevant clinical factors, even small amounts of myocardial injury (e.g., troponin I >0.03 to 0.09 ng/ml; n = 455; 16.6%) were significantly associated with death (adjusted hazard ratio: 1.75; 95% CI: 1.37 to 2.24; p < 0.001) while greater amounts (e.g., troponin I >0.09 ng/dl; n = 530; 19.4%) were significantly associated with higher risk (adjusted HR: 3.03; 95% CI: 2.42 to 3.80; p < 0.001).
Conclusions: Myocardial injury is prevalent among patients hospitalized with COVID-19; however, troponin concentrations were generally present at low levels. Patients with CVD are more likely to have myocardial injury than patients without CVD. Troponin elevation among patients hospitalized with COVID-19 is associated with higher risk of mortality.
Keywords: COVID-19; coronavirus; myocardial injury; troponin.
Published by Elsevier Inc.
Figures
Update of
-
Prevalence and Impact of Myocardial Injury in Patients Hospitalized with COVID-19 Infection.medRxiv [Preprint]. 2020 Apr 24:2020.04.20.20072702. doi: 10.1101/2020.04.20.20072702. medRxiv. 2020. Update in: J Am Coll Cardiol. 2020 Aug 4;76(5):533-546. doi: 10.1016/j.jacc.2020.06.007. PMID: 32511658 Free PMC article. Updated. Preprint.
Comment in
-
Myocardial injury in patients with COVID-19.Nat Rev Cardiol. 2020 Aug;17(8):454. doi: 10.1038/s41569-020-0408-6. Nat Rev Cardiol. 2020. PMID: 32572194 Free PMC article.
-
Myocardial Injury in COVID-19 Patients: The Beginning or the End?J Am Coll Cardiol. 2020 Aug 4;76(5):547-549. doi: 10.1016/j.jacc.2020.06.045. J Am Coll Cardiol. 2020. PMID: 32731932 Free PMC article.
-
What Happened to Electrocardiogram as a Screening Test to Recognize Cardiovascular Complications in COVID-19 Patients?J Am Coll Cardiol. 2020 Dec 8;76(23):2799-2800. doi: 10.1016/j.jacc.2020.09.611. J Am Coll Cardiol. 2020. PMID: 33272378 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
