

Transplanting neural progenitor cells to restore connectivity after spinal cord injury
- PMID: 32518349
- PMCID: PMC8384139
- DOI: 10.1038/s41583-020-0314-2
Transplanting neural progenitor cells to restore connectivity after spinal cord injury
Abstract
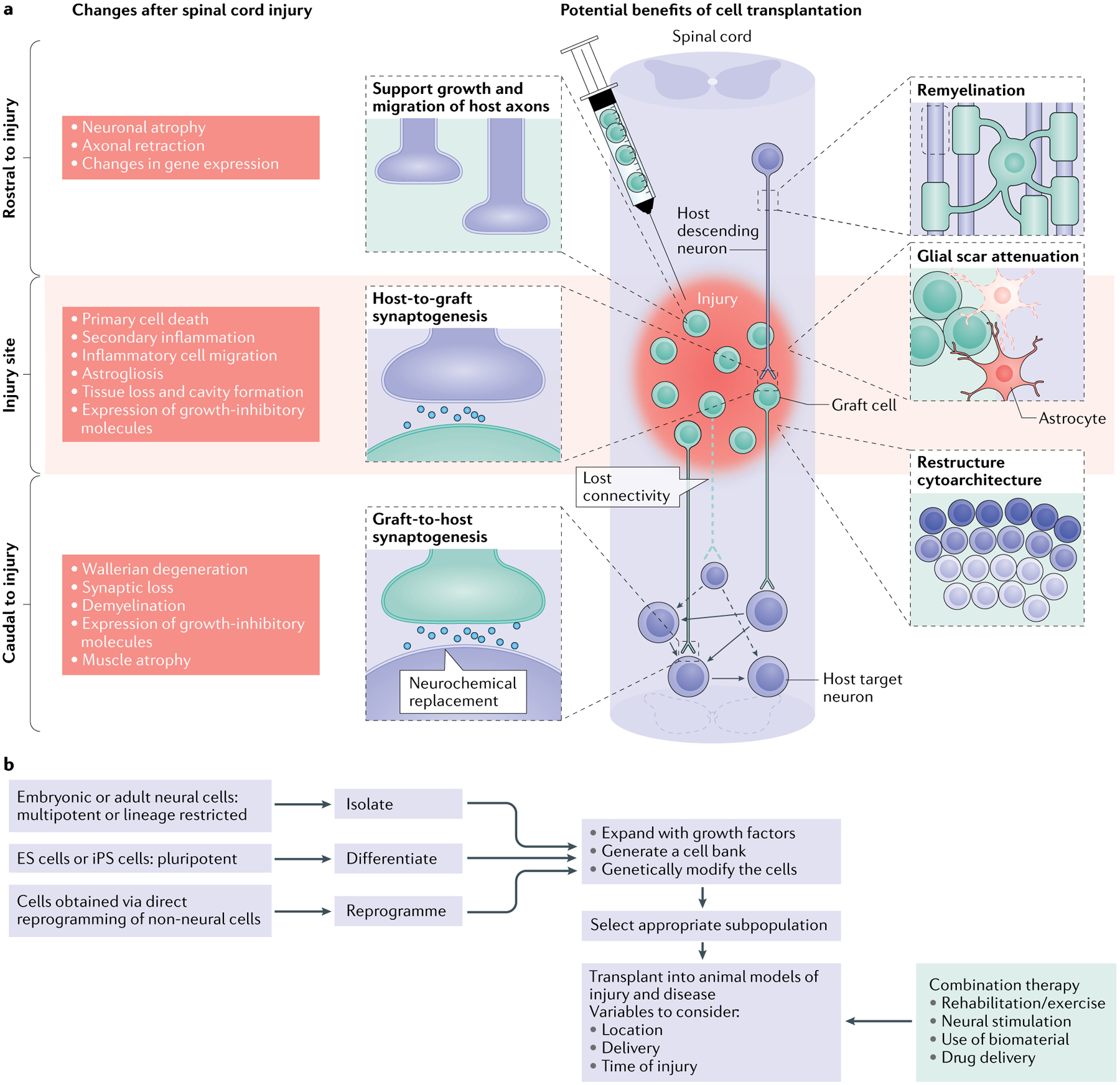
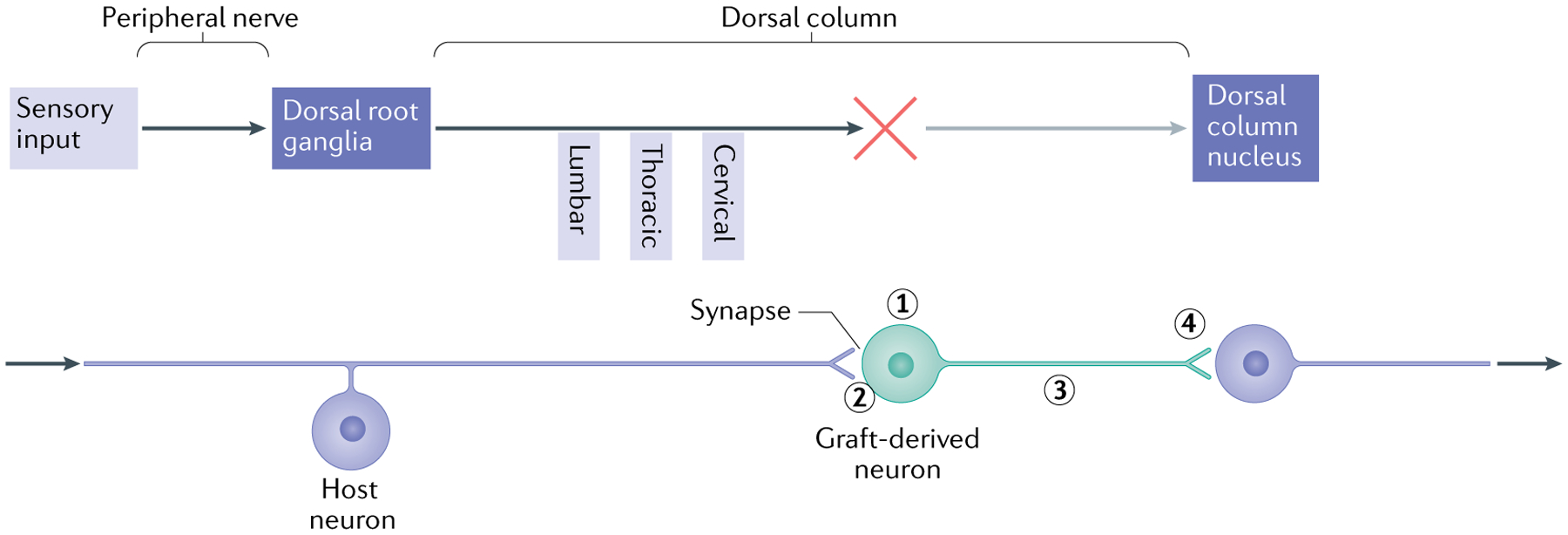
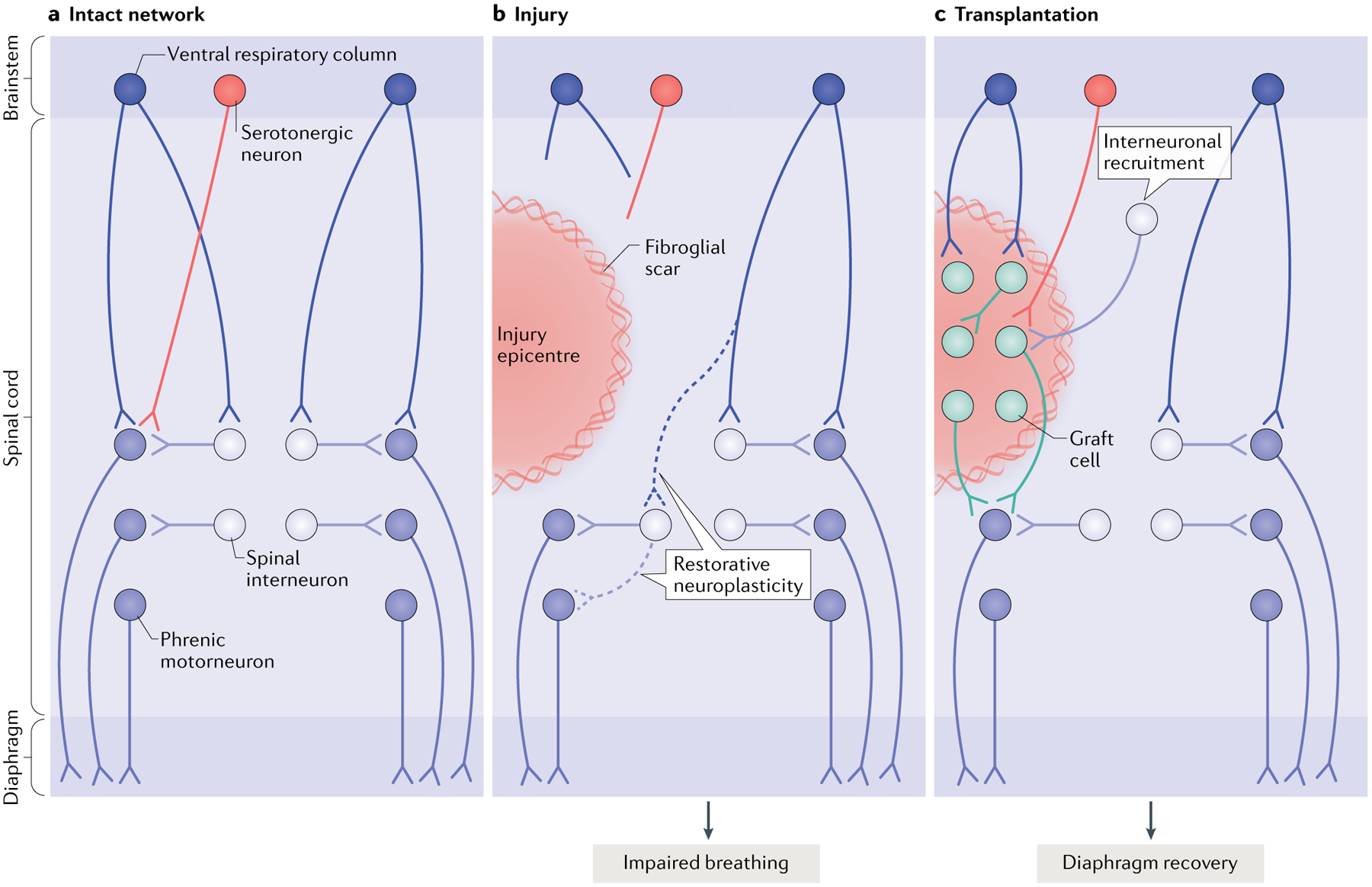
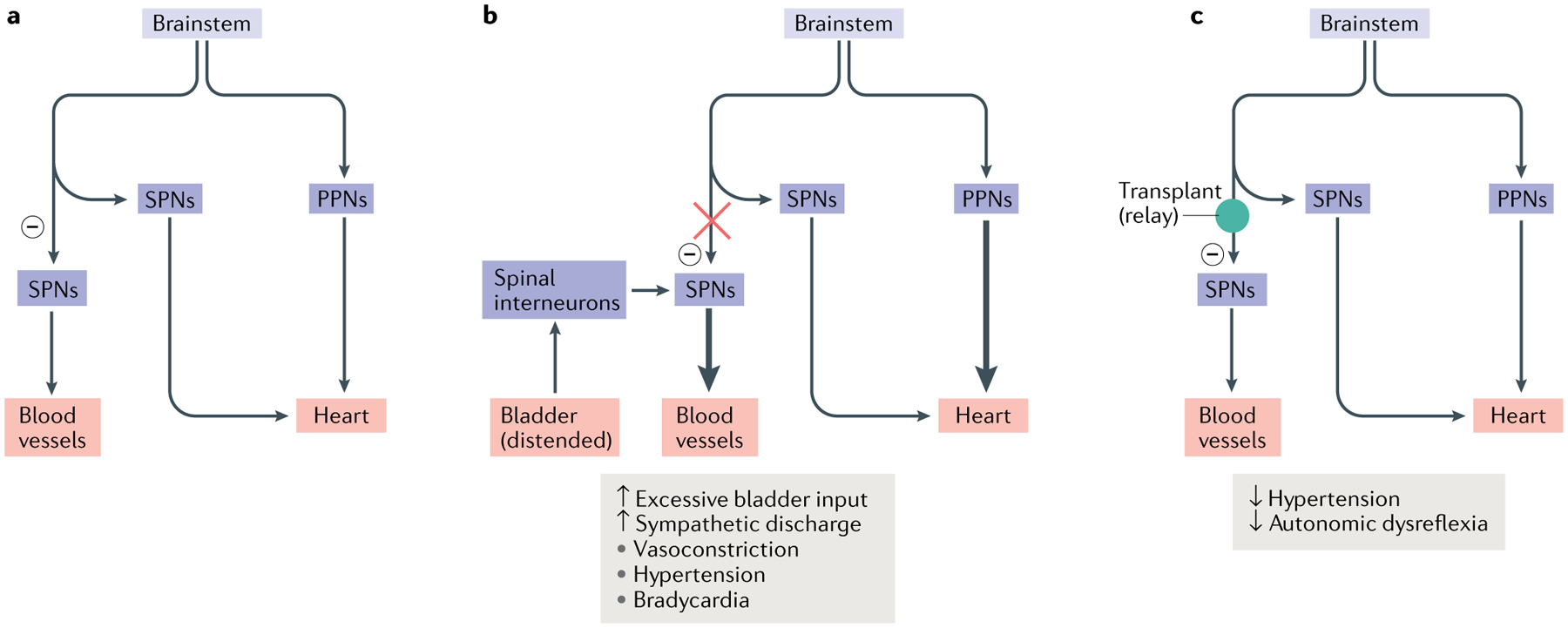
Spinal cord injury remains a scientific and therapeutic challenge with great cost to individuals and society. The goal of research in this field is to find a means of restoring lost function. Recently we have seen considerable progress in understanding the injury process and the capacity of CNS neurons to regenerate, as well as innovations in stem cell biology. This presents an opportunity to develop effective transplantation strategies to provide new neural cells to promote the formation of new neuronal networks and functional connectivity. Past and ongoing clinical studies have demonstrated the safety of cell therapy, and preclinical research has used models of spinal cord injury to better elucidate the underlying mechanisms through which donor cells interact with the host and thus increase long-term efficacy. While a variety of cell therapies have been explored, we focus here on the use of neural progenitor cells obtained or derived from different sources to promote connectivity in sensory, motor and autonomic systems.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures
Comment in
-
What the Editors are reading - Basic science.J Pediatr Urol. 2021 Apr;17(2):271-272. doi: 10.1016/j.jpurol.2020.12.010. Epub 2020 Dec 10. J Pediatr Urol. 2021. PMID: 33358556 No abstract available.
References
-
- Ahuja CS et al.Traumatic spinal cord injury. Nat. Rev. Dis. Prim 3, 17018 (2017). - PubMed
-
- Mautes AE, Weinzierl MR, Donovan F & Noble LJ Vascular events after spinal cord injury: contribution to secondary pathogenesis. Phys. Ther 80, 673–687 (2000). - PubMed
-
- Beattie MS Inflammation and apoptosis: linked therapeutic targets in spinal cord injury. Trends Mol. Med 10, 580–583 (2004). - PubMed
-
- Jia Z et al.Oxidative stress in spinal cord injury and antioxidant-based intervention. Spinal Cord 50, 264–274 (2012). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
