

Nonalcoholic fatty liver disease and type 2 diabetes: where do Diabetologists stand?
- PMID: 32518675
- PMCID: PMC7275502
- DOI: 10.1186/s40842-020-00097-1
Nonalcoholic fatty liver disease and type 2 diabetes: where do Diabetologists stand?
Abstract
Background: Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease worldwide. The increasing prevalence of NAFLD mirrors that of obesity and type 2 diabetes over the last two decades.
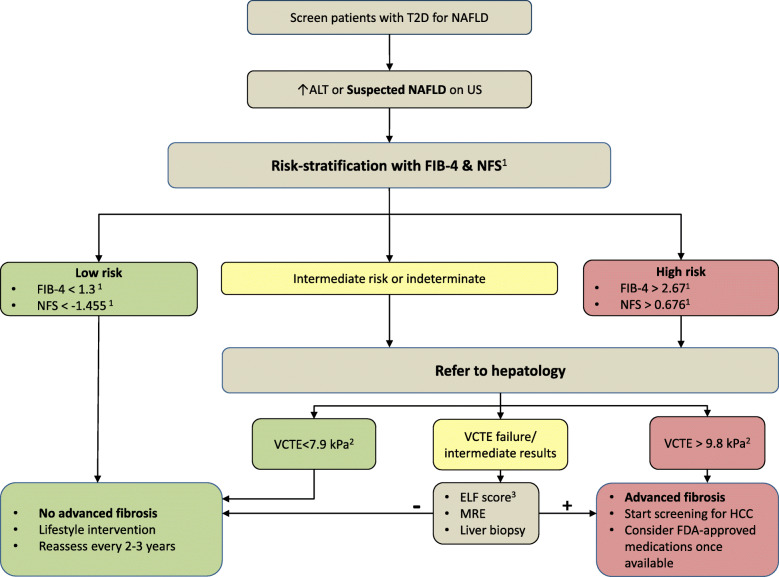
Main: In a two-way pathophysiologic relationship, NAFLD increases the risk of developing type 2 diabetes, while the latter promotes the progression of simple fatty liver to a more advanced form called nonalcoholic steatohepatitis (NASH). NASH increases the risk of cirrhosis and hepatocellular carcinoma (HCC), which may require liver transplantation. With the absence of FDA-approved medications for NAFLD treatment, lifestyle intervention remains the only therapy. Lately, extensive research efforts have been aimed at modifying NASH fibrosis and developing noninvasive screening methods.
Conclusion: We highlight the pathophysiologic relationships between NAFLD and type 2 diabetes, discuss disease recognition, models of care, and current and emerging therapies for NASH treatment.
Keywords: Awareness; Nonalcoholic fatty liver disease; Nonalcoholic steatohepatitis; Pathophysiology; Screening; Treatment; Type 2 diabetes.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsS.T. has nothing to disclose. N.A. advises, is on the speakers’ bureau for, and received grants from Gilead and Intercept. He advises and received grants from Allergan. He received grants from GENFIT, Madrigal, and Galmed. O.H. reports consultation to Abbott Nutrition, Gilead Inc. and Merck Sorono, grants from National Dairy Council, and own shares in Heathimation Inc. outside the submitted work.
Figures


References
-
- Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the Study of Liver Diseases. Hepatology. 2018;67(1):328–357. - PubMed
-
- Crespo M, Lappe S, Feldstein AE, Alkhouri N. Similarities and differences between pediatric and adult nonalcoholic fatty liver disease. Metabol Clin Exp. 2016;65(8):1161–1171. - PubMed
-
- Masarone M, Federico A, Abenavoli L, Loguercio C, Persico M. Non alcoholic fatty liver: epidemiology and natural history. Rev Recent Clin Trials. 2014;9(3):126–133. - PubMed
-
- Lonardo A, Bellentani S, Argo CK, Ballestri S, Byrne CD, Caldwell SH, et al. Epidemiological modifiers of non-alcoholic fatty liver disease: focus on high-risk groups. Dig Liver Dis. 2015;47(12):997–1006. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
