

Hyperpyrexia in patients with COVID-19
- PMID: 32519768
- PMCID: PMC7300797
- DOI: 10.1002/jmv.26154
Hyperpyrexia in patients with COVID-19
Abstract
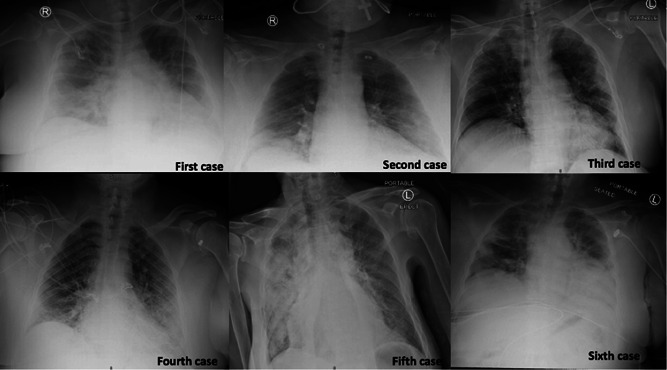
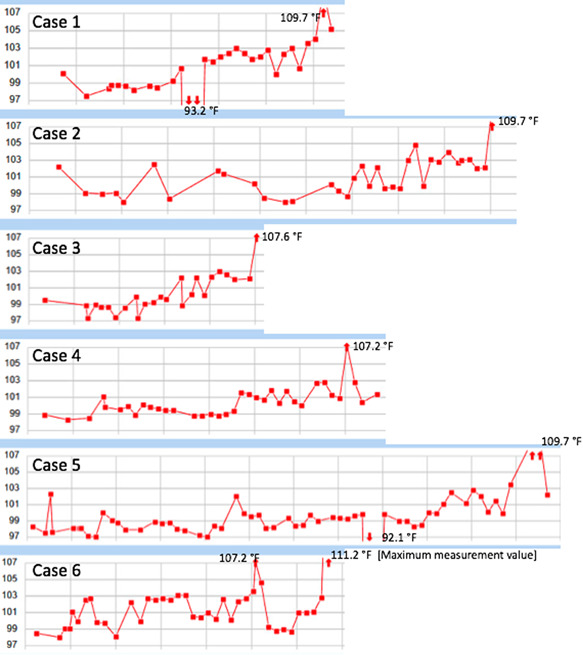
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a global health emergency, in which its effective treatment and prevention remain obscured. Hyperpyrexia is an elevation of body temperature above 106.7°F (41.5°C) due to an abnormally increased hypothalamic-thermoregulatory set. The pathophysiology, impact, and outcomes of hyperpyrexia in patients with COVID-19 have not yet been studied. Herein, we present clinical features and outcomes of six patients with COVID-19 who had developed hyperpyrexia during hospitalization. All patients expired shortly after the onset of hyperpyrexia. Hyperpyrexia seems to adversely impact the outcomes and mortality in patients with COVID-19. The underlying mechanisms of developing hyperpyrexia in COVID-19 are mysterious. We propose it may be caused by SARS-CoV-2-related brain injury, exuberant immune response, and thrombus formation. More research is needed to verify our results. Understanding the association between hyperpyrexia and SARS-CoV-2 will help to elucidate the COVID-19 pathogenesis, which is mandatory for developing effective treatment strategies.
Keywords: COVID; SARS-CoV-2; fever; hyperpyrexia.
© 2020 Wiley Periodicals LLC.
Conflict of interest statement
The authors declare that there are no conflict of interests.
Figures
Comment in
-
Hyperpyrexia and metabolic alkalosis in a COVID-19 patient.J Med Virol. 2021 Jan;93(1):176. doi: 10.1002/jmv.26276. Epub 2020 Jul 15. J Med Virol. 2021. PMID: 32639623 Free PMC article. No abstract available.
References
-
- WHO Coronavirus disease 2019 (COVID‐19) situation report—132. https://www.who.int/docs/default-source/coronaviruse/situation-reports/2.... Accessed 31 May 2020.
-
- Wu C, Chen X, Cai Y, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan. China. JAMA Intern Med. 2020. https://10.1001/jamainternmed.2020.0994 - DOI - PMC - PubMed
-
- Loscalzo J, Fauci A, Braunwald E, Dennis KL, Hauser SL, Longo DL. Chapter 17: fever versus hyperthermia. Harrison's Principles of Internal Medicine. New York, NY: McGraw‐Hill Medical; 2008.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
