

Impact of the systemic immune-inflammation index for the prediction of prognosis and modification of the risk model in patients with metastatic renal cell carcinoma treated with first-line tyrosine kinase inhibitors
- PMID: 32520703
- PMCID: PMC7673821
- DOI: 10.5489/cuaj.6413
Impact of the systemic immune-inflammation index for the prediction of prognosis and modification of the risk model in patients with metastatic renal cell carcinoma treated with first-line tyrosine kinase inhibitors
Erratum in
-
Erratum.Can Urol Assoc J. 2021 Jun;15(6):E329. doi: 10.5489/cuaj.7433. Can Urol Assoc J. 2021. PMID: 34127185 Free PMC article. No abstract available.
Abstract
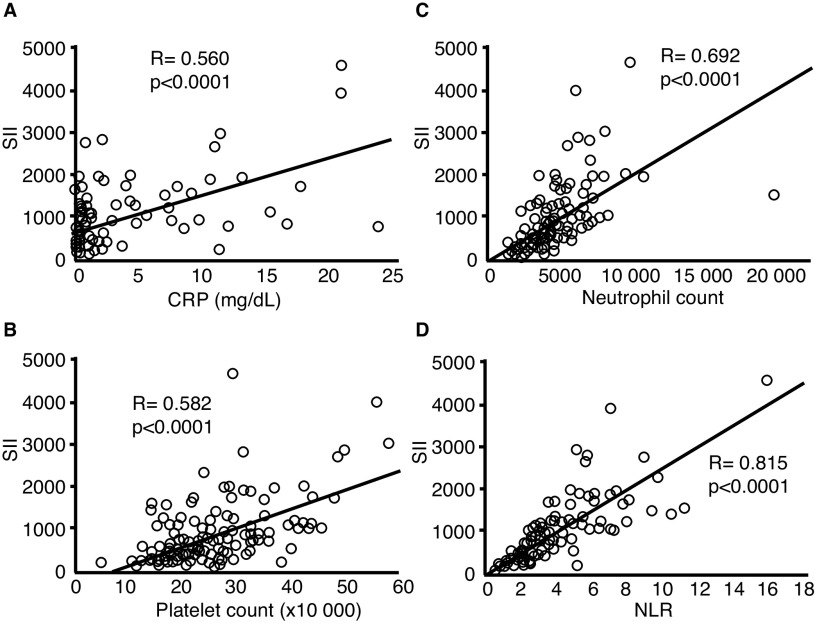
Introduction: International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) criteria are the most representative risk model for patients with metastatic renal cell carcinoma (mRCC). However, the intermediate-risk group of IMDC criteria is thought to include patients with different prognoses because many of the patients are classified into the intermediate-risk group. In this study, we investigated the impact of systemic immune-inflammation index (SII), which is calculated based on neutrophil count, platelet count, and lymphocyte count, on predicting the prognosis in patients with mRCC, and its usefulness for re-classification of patients with a more sophisticated risk model.
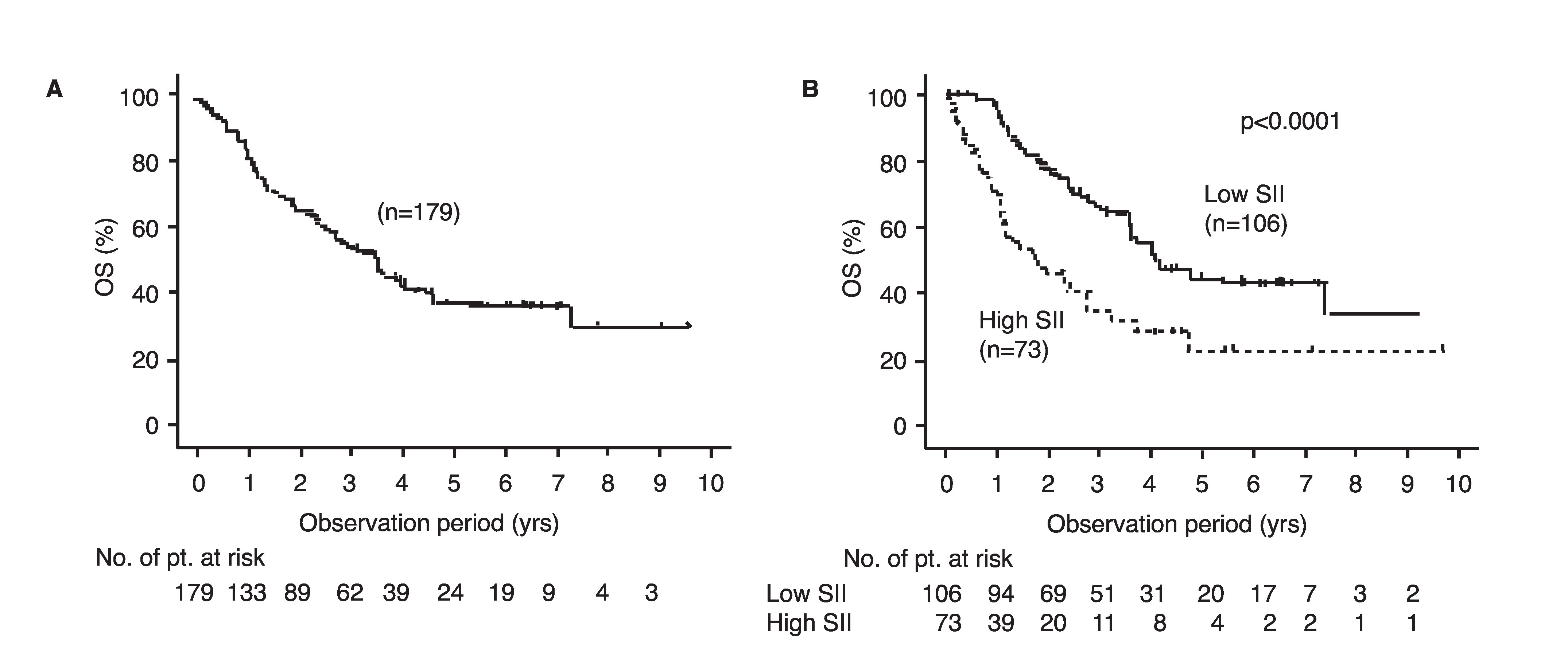
Methods: From January 2008 to January 2018, 179 mRCC patients with a pretreatment and SII were retrospectively investigated. All patients were classified into either a high-SII group or a low-SII group based on the cutoff value of a SII at 730, as reported in previous studies; the overall survival (OS) rates in each group were compared.
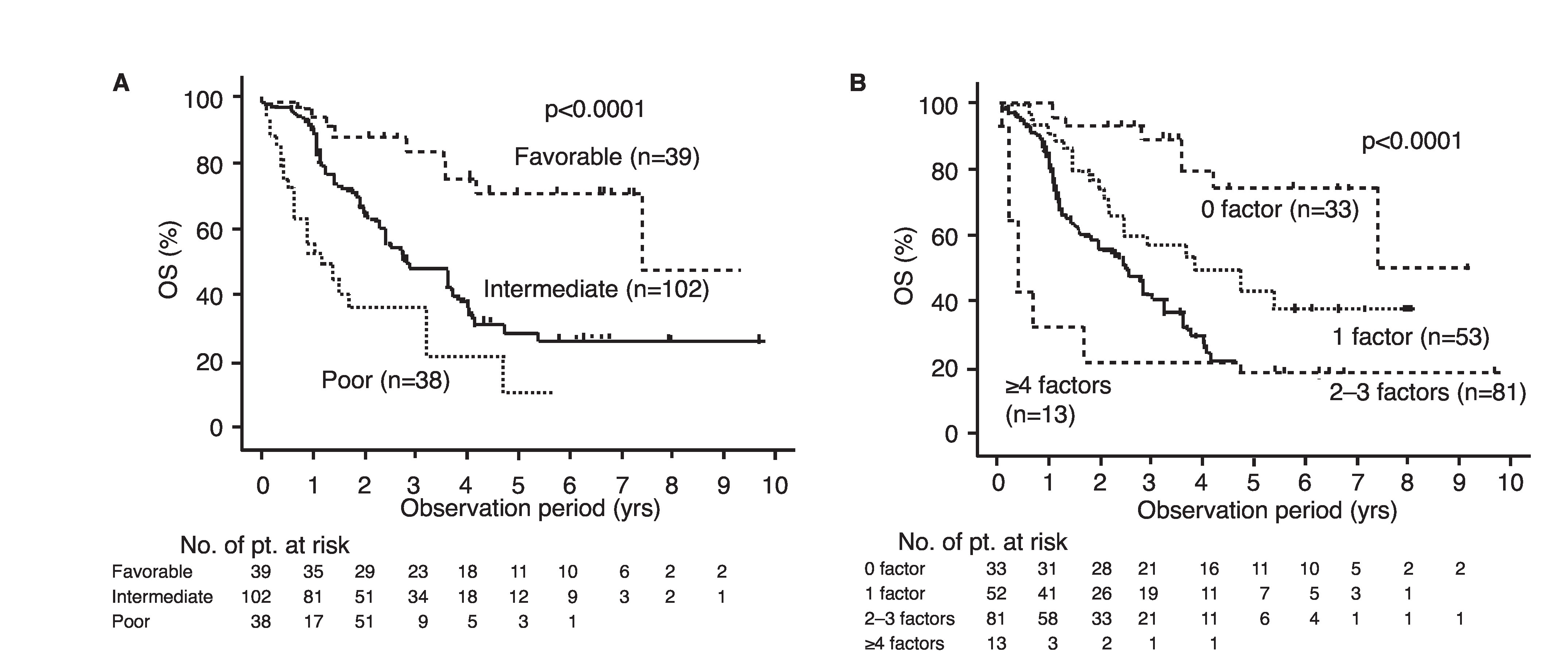
Results: The median age was 65 years old. Males and females comprised 145 and 34 cases, respectively. The categories of favorable-, intermediate-, and poor-risk groups in the IMDC model were assessed in 39, 102, and 38 cases, respectively. The median observation period was 24 months. The low-SII and high-SII groups consisted of 73 and 106 cases, respectively. The 50% OS in the high-SII group was 21.4 months, which was significantly worse than that in the low-SII group (49.7 months; p<0.0001). Multivariate analysis showed that a high SII was an independent predictive factor for a worse OS. Next, we constructed a modified IMDC risk model that included the SII instead of a neutrophil count and a platelet count. By using this modified IMDC model, all cases were re-classified into four groups of 33, 52, 81, and 13 cases with 50% OS of 88.8, 45.9, 29.4, and 4.8 months, respectively.
Conclusions: The SII is useful for establishing a more sophisticated prognostic model that can stratify mRCC patients into four groups with different prognoses.
Conflict of interest statement
Figures
References
-
- NCCN. [Accessed June 5, 2020]. Available at: https://www.nccn.org.
LinkOut - more resources
Full Text Sources
