

The Regimen of Computed Tomography Screening for Lung Cancer: Lessons Learned Over 25 Years From the International Early Lung Cancer Action Program
- PMID: 32520848
- PMCID: PMC7771636
- DOI: 10.1097/RTI.0000000000000538
The Regimen of Computed Tomography Screening for Lung Cancer: Lessons Learned Over 25 Years From the International Early Lung Cancer Action Program
Abstract
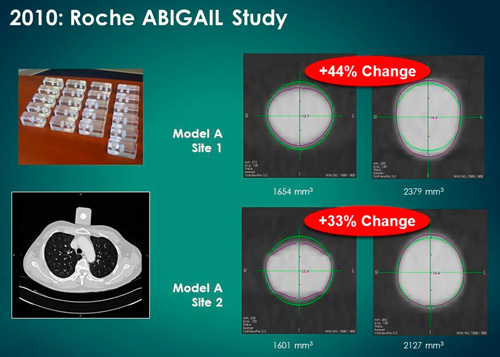
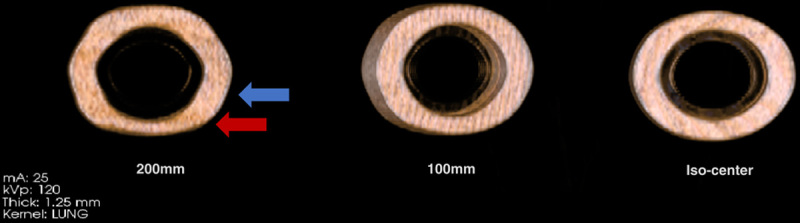
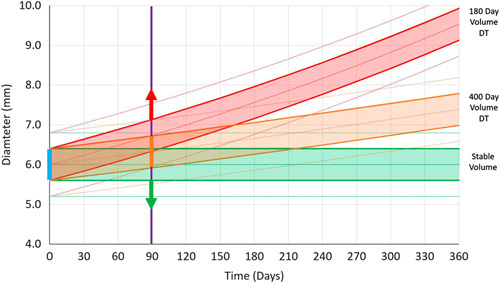
We learned many unanticipated and valuable lessons since we started planning our study of low-dose computed tomography (CT) screening for lung cancer in 1991. The publication of the baseline results of the Early Lung Cancer Action Project (ELCAP) in Lancet 1999 showed that CT screening could identify a high proportion of early, curable lung cancers. This stimulated large national screening studies to be quickly started. The ELCAP design, which provided evidence about screening in the context of a clinical program, was able to rapidly expand to a 12-institution study in New York State (NY-ELCAP) and to many international institutions (International-ELCAP), ultimately working with 82 institutions, all using the common I-ELCAP protocol. This expansion was possible because the investigators had developed the ELCAP Management System for screening, capturing data and CT images, and providing for quality assurance. This advanced registry and its rapid accumulation of data and images allowed continual assessment and updating of the regimen of screening as advances in knowledge and new technology emerged. For example, in the initial ELCAP study, introduction of helical CT scanners had allowed imaging of the entire lungs in a single breath, but the images were obtained in 10 mm increments resulting in about 30 images per person. Today, images are obtained in submillimeter slice thickness, resulting in around 700 images per person, which are viewed on high-resolution monitors. The regimen provides the imaging acquisition parameters, imaging interpretation, definition of positive result, and the recommendations for further workup, which now include identification of emphysema and coronary artery calcifications. Continual updating is critical to maximize the benefit of screening and to minimize potential harms. Insights were gained about the natural history of lung cancers, identification and management of nodule subtypes, increased understanding of nodule imaging and pathologic features, and measurement variability inherent in CT scanners. The registry also provides the foundation for assessment of new statistical techniques, including artificial intelligence, and integration of effective genomic and blood-based biomarkers, as they are developed.
Conflict of interest statement
Dr D.F.Y. is a named inventor on a number of patents and patent applications relating to the evaluation of diseases of the chest including measurement of nodules. Some of these, which are owned by Cornell Research Foundation (CRF), are nonexclusively licensed to General Electric. As an inventor of these patents, Dr. D.F.Y. is entitled to a share of any compensation that CRF may receive from its commercialization of these patents. He is also an equity owner in Accumetra, a privately held technology company committed to improving the science and practice of image-based decision making. Dr D.F.Y. also serves on the advisory board of GRAIL. Dr C.I.H. is the President and serves on the board of the Early Diagnosis and Treatment Research Foundation. She receives no compensation from the Foundation. The Foundation is established to provide grants for projects, conferences, and public databases for research on early diagnosis and treatment of diseases. Dr C.I.H. is also a named inventor on a number of patents and patent applications relating to the evaluation of pulmonary nodules on CT scans of the chest, which are owned by Cornell Research Foundation (CRF). Since 2009, Dr C.I.H. does not accept any financial benefit from these patents including royalties and any other proceeds related to the patents or patent applications owned by CRF. The remaining authors declare no conflicts of interest.
Figures
References
-
- Henschke CI, Yankelevitz DF, Reeves AP, et al. Evolution of lung cancer screening management. Oncology (Williston Park). 2019;33:629380. - PubMed
-
- Henschke C, Boffetta P, Yankelevitz D, et al. Computed tomography screening: the international early lung cancer action program experience. Thorac Surg Clin. 2015;25:129–143. - PubMed
-
- Henschke CI, Miettinen OS, Yankelevitz DF, et al. Radiographic screening for cancer proposed paradigm for requisite research. Clin Imaging. 1994;18:16–20. - PubMed
-
- Henschke C, Caro J, Libby D, et al. Radiographic screening for lung cancer: proposed paradigm for requisite research. Clin Imaging. 1994;18:16–20. - PubMed
-
- Henschke C, Smith J, Libby D, et al. New Concepts for Lung Cancer Screening: Paradigm For Outcomes Research. Seattle, WA: American Thoracic Society; 1995:21–24.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
