

Pulmonary hypertension in bronchopulmonary dysplasia
- PMID: 32521539
- PMCID: PMC7979539
- DOI: 10.1038/s41390-020-0993-4
Pulmonary hypertension in bronchopulmonary dysplasia
Abstract
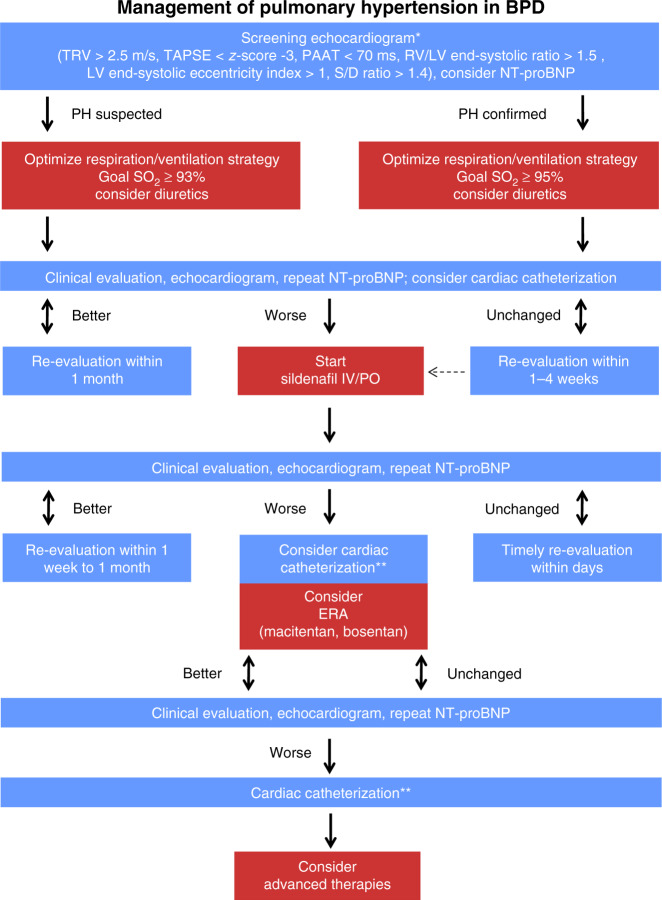
Bronchopulmonary dysplasia (BPD) is a major complication in prematurely born infants. Pulmonary hypertension (PH) associated with BPD (BPD-PH) is characterized by alveolar diffusion impairment, abnormal vascular remodeling, and rarefication of pulmonary vessels (vascular growth arrest), which lead to increased pulmonary vascular resistance and right heart failure. About 25% of infants with moderate to severe BPD develop BPD-PH that is associated with high morbidity and mortality. The recent evolution of broader PH-targeted pharmacotherapy in adults has opened up new treatment options for infants with BPD-PH. Sildenafil became the mainstay of contemporary BPD-PH therapy. Additional medications, such as endothelin receptor antagonists and prostacyclin analogs/mimetics, are increasingly being investigated in infants with PH. However, pediatric data from prospective or randomized controlled trials are still sparse. We discuss comprehensive diagnostic and therapeutic strategies for BPD-PH and briefly review the relevant differential diagnoses of parenchymal and interstitial developmental lung diseases. In addition, we provide a practical framework for the management of children with BPD-PH, incorporating the modified definition and classification of pediatric PH from the 2018 World Symposium on Pulmonary Hypertension, and the 2019 EPPVDN consensus recommendations on established and newly developed therapeutic strategies. Finally, current gaps of knowledge and future research directions are discussed. IMPACT: PH in BPD substantially increases mortality. Treatment of BPD-PH should be conducted by an interdisciplinary team and follow our new treatment algorithm while still kept tailored to the individual patient. We discuss recent developments in BPD-PH, make recommendations on diagnosis, monitoring and treatment of PH in BPD, and address current gaps of knowledge and potential research directions. We provide a practical framework, including a new treatment algorithm, for the management of children with BPD-PH, incorporating the modified definition and classification of pediatric PH (2018 WSPH) and the 2019 EPPVDN consensus recommendations on established and newly developed therapeutic strategies for BPD-PH.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Lignelli E, Palumbo F, Myti D, Morty RE. Recent advances in our understanding of the mechanisms of lung alveolarization and bronchopulmonary dysplasia. Am. J. Physiol. Lung Cell. Mol. Physiol. 2019;317:L832–L887. - PubMed
-
- Weismann CG, et al. Pulmonary hypertension in preterm infants: results of a prospective screening program. J. Perinatol. 2017;37:572–577. - PubMed
-
- Khemani E, et al. Pulmonary artery hypertension in formerly premature infants with bronchopulmonary dysplasia: clinical features and outcomes in the surfactant era. Pediatrics. 2007;120:1260–1269. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
