

Efficacy and safety of sarilumab in combination with csDMARDs or as monotherapy in subpopulations of patients with moderately to severely active rheumatoid arthritis in three phase III randomized, controlled studies
- PMID: 32522251
- PMCID: PMC7288435
- DOI: 10.1186/s13075-020-02194-z
Efficacy and safety of sarilumab in combination with csDMARDs or as monotherapy in subpopulations of patients with moderately to severely active rheumatoid arthritis in three phase III randomized, controlled studies
Abstract
Background: The interleukin-6 receptor inhibitor sarilumab demonstrated efficacy in combination with conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) or as monotherapy in patients with moderately to severely active rheumatoid arthritis (RA) with an inadequate response (IR) or intolerant (INT) to methotrexate (MTX) or tumour necrosis factor (TNF)-α inhibitors. This analysis investigated the efficacy and safety of sarilumab in patient subgroups.
Methods: Data were included from phase III studies: two placebo-controlled studies of subcutaneous sarilumab 150/200 mg every 2 weeks (q2w) either + MTX in MTX-IR patients (52 weeks) or + csDMARDs in TNF-IR/INT patients (24 weeks), and a monotherapy study of sarilumab 200 mg q2w vs. adalimumab 40 mg q2w in MTX-IR/INT patients (24 weeks). Prespecified and post hoc subgroups included patient demographics, disease characteristics, and prior treatments. Prespecified and post hoc endpoints included clinical, radiographic, and physical function measures, and p values are considered nominal. Safety was assessed during double-blind treatment.
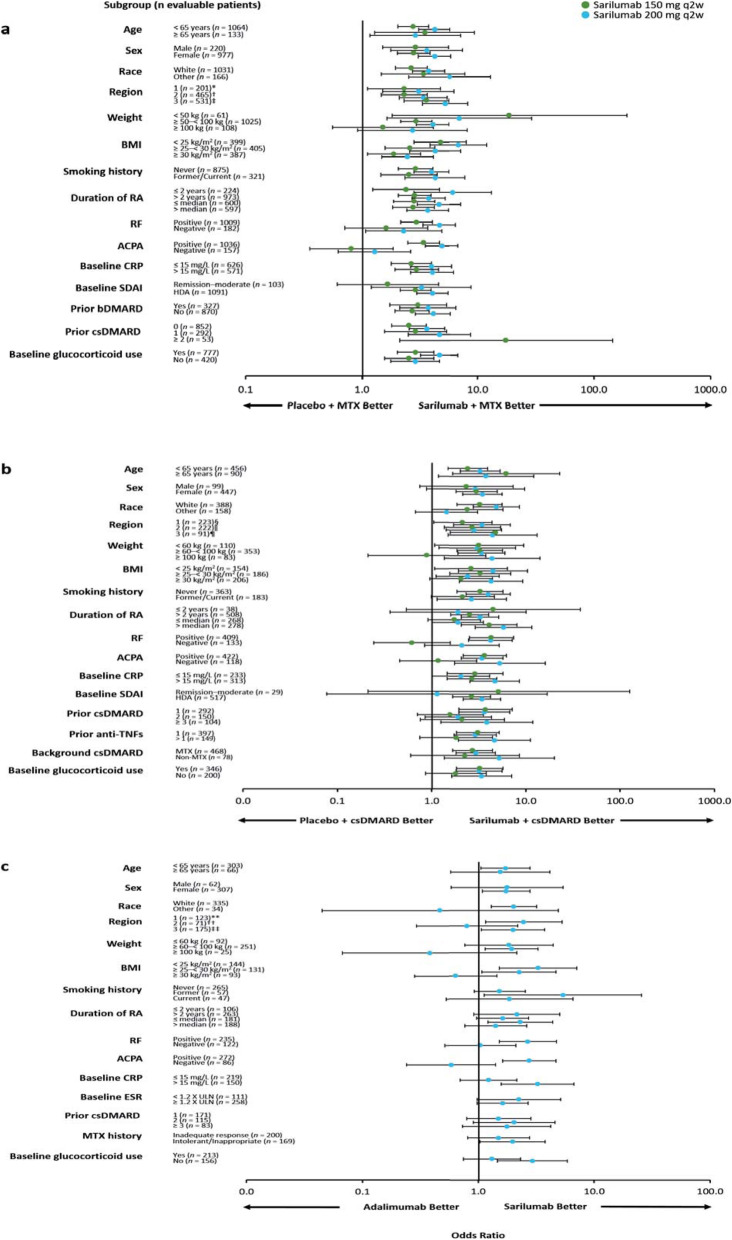
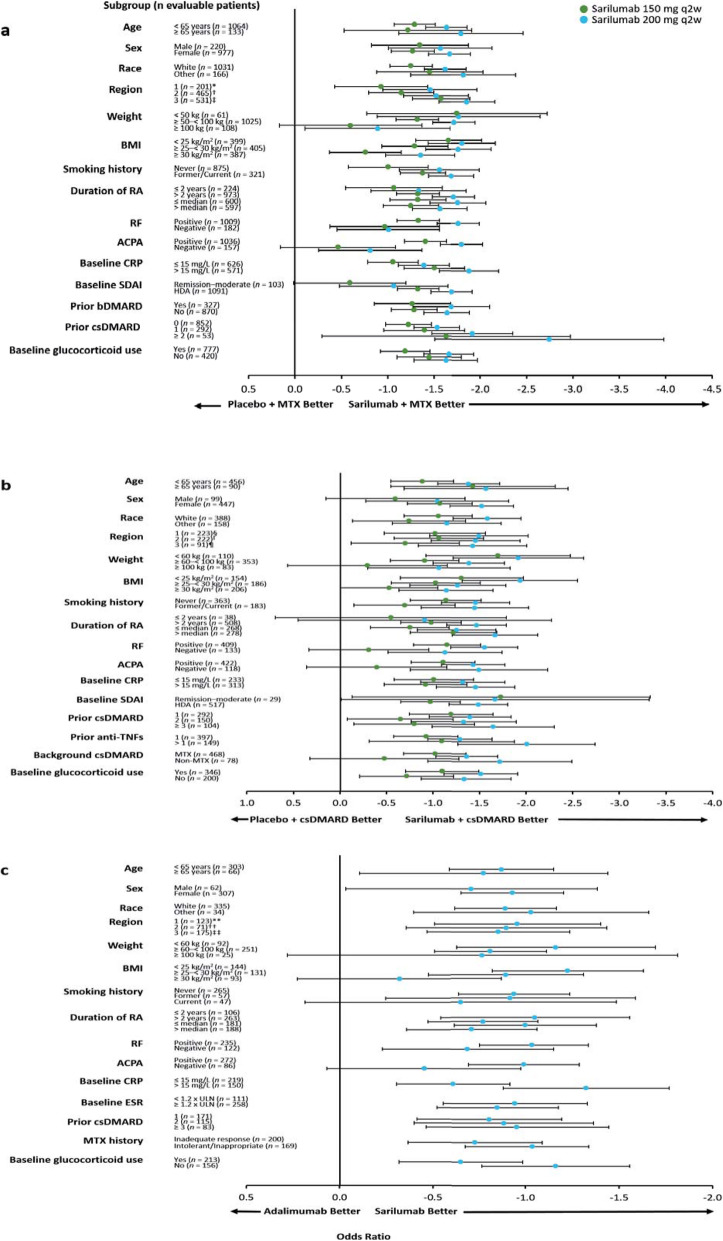
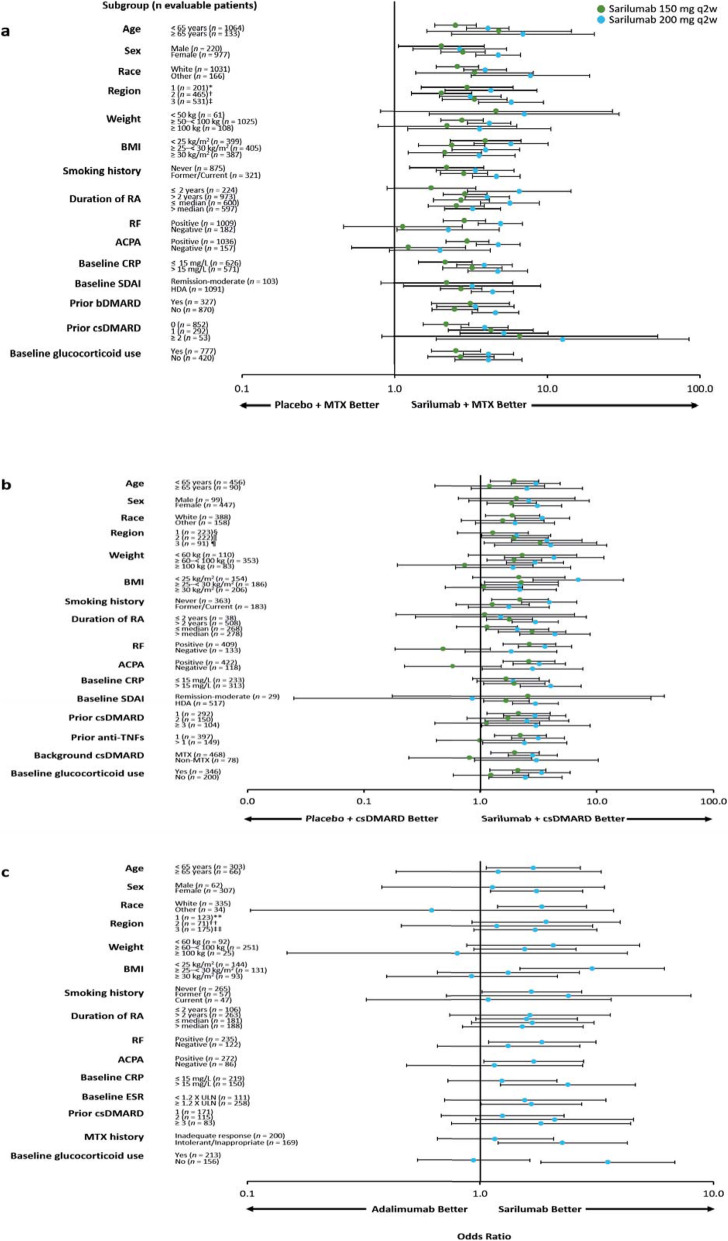
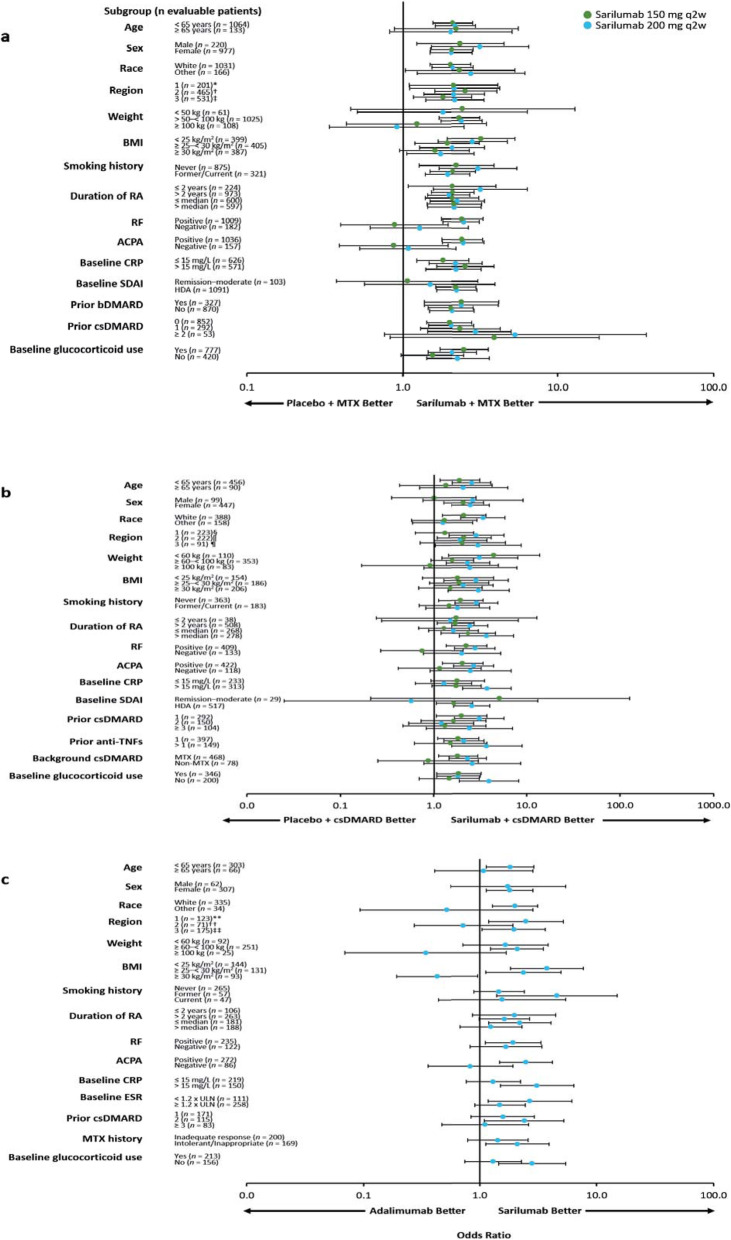
Results: The superiority of sarilumab (either as monotherapy vs. adalimumab or in combination with csDMARDs vs. placebo + csDMARDs) across clinical endpoints was generally consistent across subgroups defined by patient demographics, disease characteristics, and prior treatments, demonstrating the benefit of sarilumab treatment for a wide range of patient types. Interaction p values of < 0.05 were consistently observed across studies only for baseline anti-cyclic citrullinated peptide antibody (ACPA) status for American College of Rheumatology 20% response, but not American College of Rheumatology 50% or 70% response. Adverse events and worsening laboratory parameters occurred more frequently in sarilumab-treated vs. placebo-treated patients and were more frequent in the small number of patients ≥ 65 years (n = 289) vs. patients < 65 years (n = 1819). Serious infections occurred in six patients aged ≥ 65 years receiving sarilumab, although the incidence of serious infections was generally higher in patients aged ≥ 65 years regardless of treatment.
Conclusions: Apart from ACPA status, there were no consistent signals indicating differential effects of sarilumab in any of the subpopulations assessed. Sarilumab demonstrated consistent efficacy and safety across a wide range of patients with RA.
Trial registration: ClinicalTrials.gov NCT01061736, registered on February 03, 2010; ClinicalTrials.gov NCT01709578, registered on October 18, 2012; ClinicalTrials.gov NCT02332590, registered on January 07, 2015.
Keywords: Adalimumab; Interleukin-6; Methotrexate; Rheumatoid arthritis; Sarilumab; Subpopulations; csDMARDs.
Conflict of interest statement
MCG has received research grants and consulting fees or other remuneration (payment) from Genentech, Roche, R-Pharm, and Sanofi Genzyme. RF has received research grants from AbbVie, Amgen, Ardea Biosciences, Bristol-Myers Squibb, Celgene, Eli Lilly, EMD Serono, GlaxoSmithKline, Novartis, Pfizer, Regeneron Pharmaceuticals, Inc., Roche, Sanofi Genzyme, and UCB, and has received consulting fees from AbbVie, Akros Pharma, Amgen, AstraZeneca, Bristol-Myers Squibb, Celltrion, Eli Lilly, GlaxoSmithKline, Janssen, Novartis, Pfizer, Roche, Sandoz, Sanofi Genzyme, Taiho Pharmaceutical, and UCB. AK has received consulting fees from Pfizer, Roche, Sanofi Genzyme, and UCB, and holds stock in Sanofi Genzyme and Regeneron Pharmaceuticals, Inc. EBL has received consulting fees from Pfizer. HvH is an employee of Sanofi Genzyme and may hold stock and/or stock options in the company. TK, GSJ, and EKM are employees of Regeneron Pharmaceuticals, Inc. and may hold stock and/or stock options in the company. GRB has received research grants from AbbVie, Pfizer, Roche, and UCB, and has received consulting fees or other remuneration (payment) or participated in speakers’ bureaus from/for AbbVie, Eli Lilly, Merck Sharp & Dohme, Pfizer, Roche, Sanofi Genzyme, and UCB.
Figures
References
-
- Global Burden of Disease Study 2017 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. - PMC - PubMed
-
- Singh JA, Saag KG, Bridges SL, Jr, Akl EA, Bannuru RR, Sullivan MC, et al. 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68(1):1–26. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
