

Is it necessary to tie the medial row in rotator cuff repair double-row constructs when using suture tape?
- PMID: 32523297
- PMCID: PMC7275275
- DOI: 10.1016/j.jcot.2020.02.007
Is it necessary to tie the medial row in rotator cuff repair double-row constructs when using suture tape?
Erratum in
-
Erratum regarding previously published articles.J Clin Orthop Trauma. 2020 Nov-Dec;11(6):1169-1171. doi: 10.1016/j.jcot.2020.09.032. Epub 2020 Sep 26. J Clin Orthop Trauma. 2020. PMID: 33013141 Free PMC article.
-
Erratum regarding previously published articles.J Clin Orthop Trauma. 2020 Nov-Dec;11(6):1172-1174. doi: 10.1016/j.jcot.2020.10.044. Epub 2020 Oct 23. J Clin Orthop Trauma. 2020. PMID: 33192025 Free PMC article.
-
Erratum regarding previously published articles.J Clin Orthop Trauma. 2021 Aug 5;21:101560. doi: 10.1016/j.jcot.2021.101560. eCollection 2021 Oct. J Clin Orthop Trauma. 2021. PMID: 34414073 Free PMC article.
Abstract
Purpose: To evaluate the selected biomechanical differences of a double-row trans-osseous equivalent rotator cuff repair with a knotless versus knot-tying medial row using suture tape in regard to repair displacement, stiffness, and ultimate load to failure.
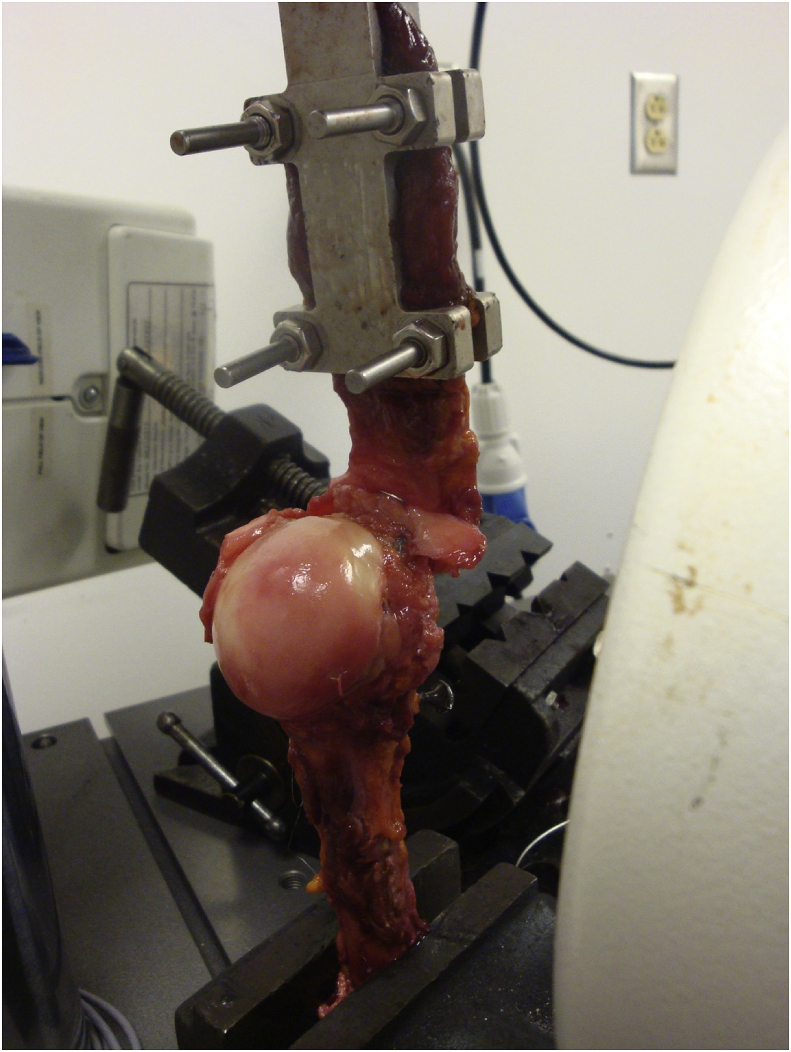
Methods: In 16 fresh-frozen human shoulders (8 matched pairs), double-row rotator cuff repairs were performed with medial-row mattress knots (MK) on one side, the other without (NK). Two DVRT (Differential Variable Reluctance Transducer) sensors were attached between the humerus and 3 mm above the repair site and were used to measure the displacement across the repair during cycling. The biomechanical parameters measured were repair displacement, stiffness, and ultimate load to failure. The supraspinatus was loaded in a similar fashion to previously described protocol using cyclic loading and load to failure testing.1.
Results: All data from paired specimens were compared using paired Student t tests. No statistically significant difference (SSD) in displacement across the repair over the 200 cycles of the test was noted between the two groups (MK = 0.591 ± 0.501 mm; NK = 0.439 ± 0.417 mm, p = 0.618). No SSD in stiffness was noted between the two groups (MK = 32.87 ± 6.31 N/mm; NK = 27.98 ± 9.69 N/mm, p = 0.120). No SSD in ultimate load to failure was noted between the two groups (MK = 501.2 ± 126.1 N; NK = 416.8 ± 120.0 N, p = 0.116).
Conclusion: There was no statistically significant different between knotless versus knotted medial row double row rotator cuff repair constructs using suture tape in regard to displacement across the repair site, stiffness and ultimate load to failure. Despite previous evidence suggesting inferiority of knotless medial row technique using suture constructs, this evidence may support the biomechanical equivalency of knotless medial row technique using suture tape.
Keywords: Double row; Knotless fixation; Rotator cuff; Suture tape.
© 2020 Delhi Orthopedic Association. All rights reserved.
Figures


References
-
- Burkhart S.S., Denard P.J., Konicek J., Hanypsiak B.T. Biomechanical validation of load-sharing rip-stop fixation for the repair of tissue-deficient rotator cuff tears. Am J Sports Med. 2014;42(2):457–462. - PubMed
-
- Vaishnav S., Millett P.J. Arthroscopic rotator cuff repair: scientific rationale, surgical technique, and early clinical and functional results of a knotless self-reinforcing double-row rotator cuff repair system. J Shoulder Elbow Surg. 2010;19(2):83–90. - PubMed
-
- Barber F.A., Drew O.R. A biomechanical comparison of tendon-bone interface motion and cyclic loading between single-row, triple-loaded cuff repairs and double-row, suture-tape cuff repairs using biocomposite anchors. Arthrosc J Arthrosc Relat Surg. 2012;28(9):1197–1205. - PubMed
-
- Denard P.J., Jiwani A.Z., Lädermann A., Burkhart S.S. Long-term outcome of arthroscopic massive rotator cuff repair: the importance of double-row fixation. Arthrosc J Arthrosc Relat Surg. 2012;28(7):909–915. - PubMed
-
- Frank J.B., ElAttrache N.S., Dines J.S., Blackburn A., Crues J., Tibone J.E. Repair site integrity after arthroscopic transosseous-equivalent suture-bridge rotator cuff repair. Am J Sports Med. 2008;36(8):1496–1503. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
