

MANIFESTATIONS OF GLUCAGONOMA SYNDROME
- PMID: 32524009
- PMCID: PMC7279770
- DOI: 10.4158/ACCR-2019-0211
MANIFESTATIONS OF GLUCAGONOMA SYNDROME
Abstract
Objective: Glucagonoma is a rare neuroendocrine tumor of the pancreas. We present the case of a young female patient who presented with the major clinical manifestations of glucagonoma syndrome.
Methods: The major clinical manifestations of glucagonoma syndrome are described in a 44-year-old, female patient. Beyond glucagonoma, the patient also displayed deep venous thrombosis, depression, diabetes, and necrolytic migratory erythema. We discuss the difficulty of treatment of patients with glucagonoma due to the low prevalence of the disorder, scarcity of medical evidence, lateness of diagnosis with liver metastases in most cases, and poor response to chemotherapy with high rates of relapse after surgery. In this case, pancreatectomy and hepatic lobectomy followed by somatostatin analogue therapy was the chosen treatment strategy.
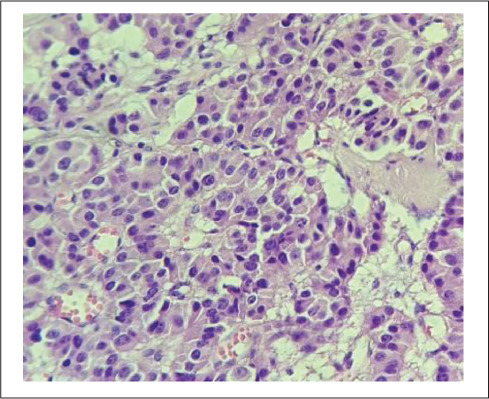
Results: The clinical findings were pancreatic and hepatic masses, proximal deep venous thrombosis, depression, diabetes, and necrolytic migratory erythema. The patient also had elevated levels of glucagon. Pancreatectomy and right hepatic lobectomy were performed and confirmed the glucagonoma.
Conclusion: Our case adds new knowledge about glucagonoma which is important due to the low incidence of the disease and the particular characteristics of the syndrome.
Copyright © 2020 AACE.
Conflict of interest statement
DISCLOSURE The authors have no multiplicity of interest to disclose.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources