

Survival After Minimally Invasive vs Open Radical Hysterectomy for Early-Stage Cervical Cancer: A Systematic Review and Meta-analysis
- PMID: 32525511
- PMCID: PMC7290695
- DOI: 10.1001/jamaoncol.2020.1694
Survival After Minimally Invasive vs Open Radical Hysterectomy for Early-Stage Cervical Cancer: A Systematic Review and Meta-analysis
Abstract
Importance: Minimally invasive techniques are increasingly common in cancer surgery. A recent randomized clinical trial has brought into question the safety of minimally invasive radical hysterectomy for cervical cancer.
Objective: To quantify the risk of recurrence and death associated with minimally invasive vs open radical hysterectomy for early-stage cervical cancer reported in observational studies optimized to control for confounding.
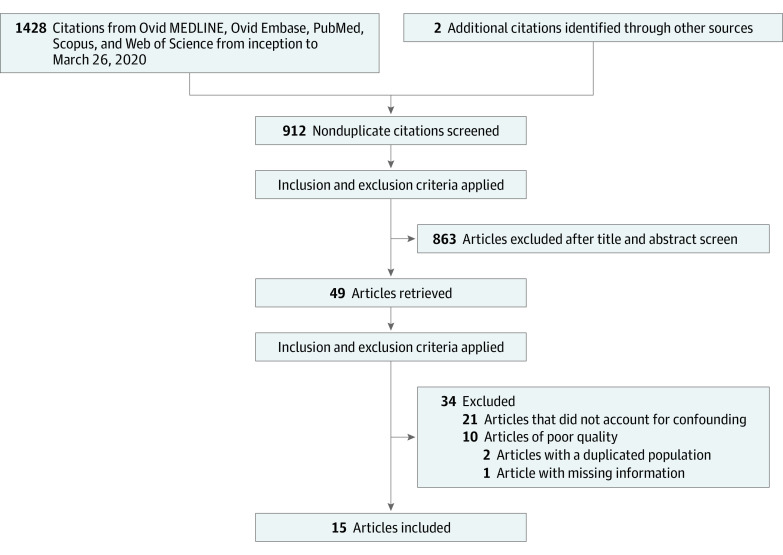
Data sources: Ovid MEDLINE, Ovid Embase, PubMed, Scopus, and Web of Science (inception to March 26, 2020) performed in an academic medical setting.
Study selection: In this systematic review and meta-analysis, observational studies were abstracted that used survival analyses to compare outcomes after minimally invasive (laparoscopic or robot-assisted) and open radical hysterectomy in patients with early-stage (International Federation of Gynecology and Obstetrics 2009 stage IA1-IIA) cervical cancer. Study quality was assessed with the Newcastle-Ottawa Scale and included studies with scores of at least 7 points that controlled for confounding by tumor size or stage.
Data extraction and synthesis: The Meta-analysis of Observational Studies in Epidemiology (MOOSE) checklist was used to abstract data independently by multiple observers. Random-effects models were used to pool associations and to analyze the association between surgical approach and oncologic outcomes.
Main outcomes and measures: Risk of recurrence or death and risk of all-cause mortality.
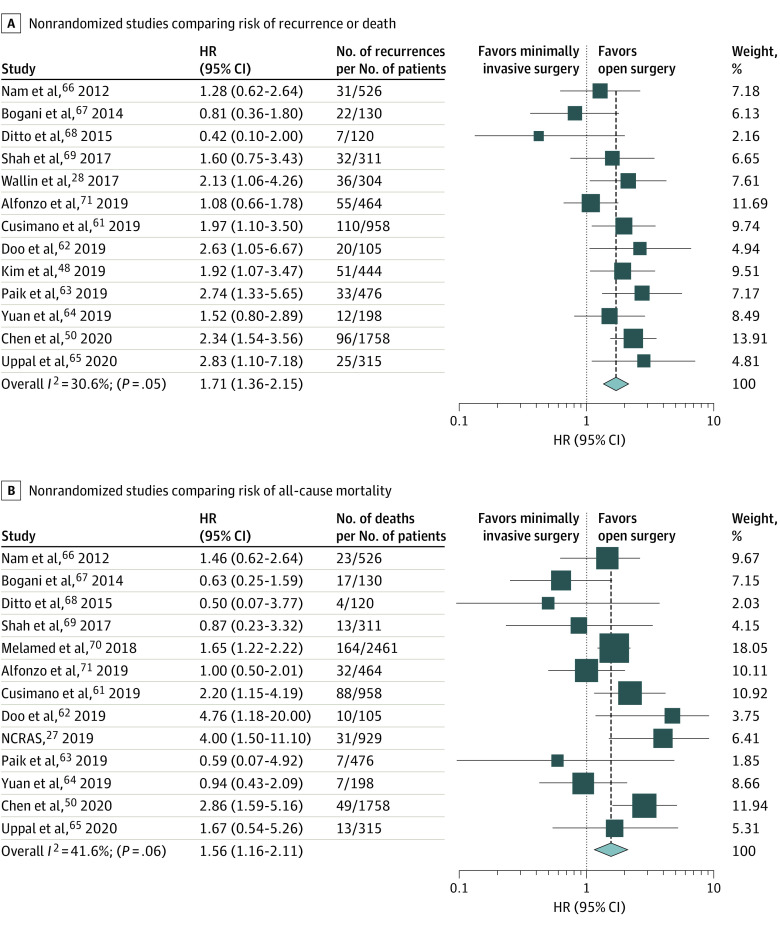
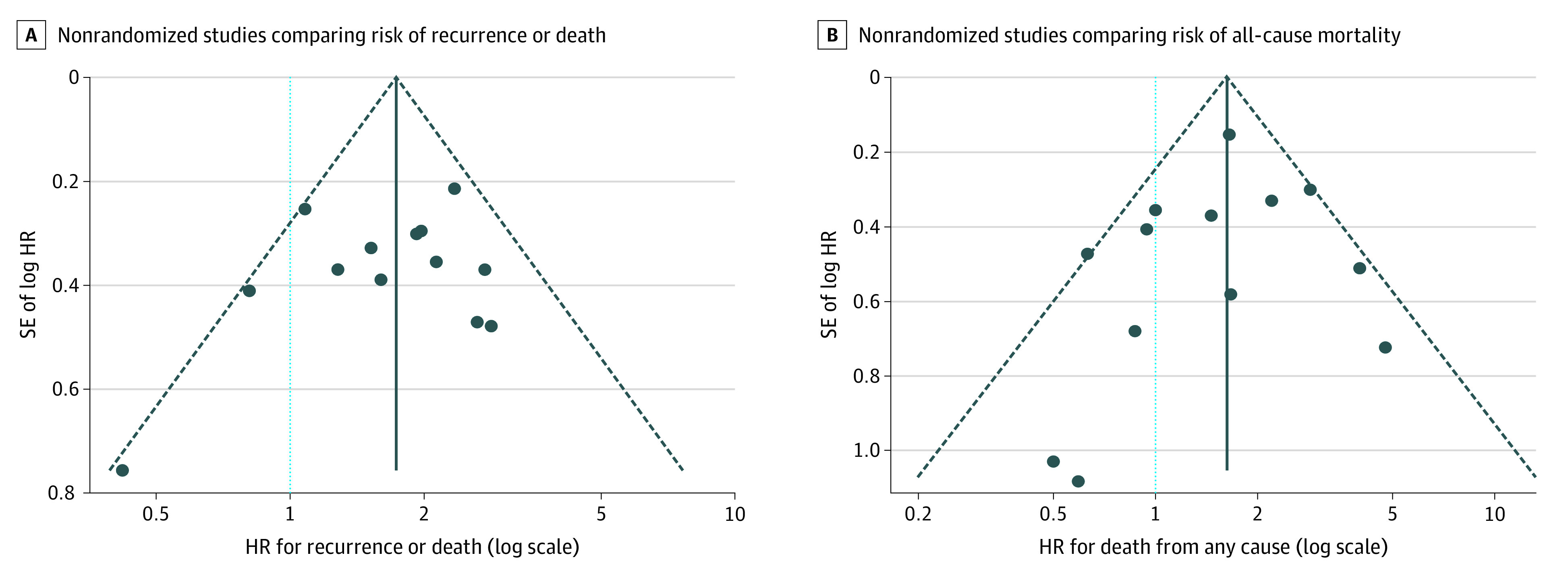
Results: Forty-nine studies were identified, of which 15 were included in the meta-analysis. Of 9499 patients who underwent radical hysterectomy, 49% (n = 4684) received minimally invasive surgery; of these, 57% (n = 2675) received robot-assisted laparoscopy. There were 530 recurrences and 451 deaths reported. The pooled hazard of recurrence or death was 71% higher among patients who underwent minimally invasive radical hysterectomy compared with those who underwent open surgery (hazard ratio [HR], 1.71; 95% CI, 1.36-2.15; P < .001), and the hazard of death was 56% higher (HR, 1.56; 95% CI, 1.16-2.11; P = .004). Heterogeneity of associations was low to moderate. No association was found between the prevalence of robot-assisted surgery and the magnitude of association between minimally invasive radical hysterectomy and hazard of recurrence or death (2.0% increase in the HR for each 10-percentage point increase in prevalence of robot-assisted surgery [95% CI, -3.4% to 7.7%]) or all-cause mortality (3.7% increase in the HR for each 10-percentage point increase in prevalence of robot-assisted surgery [95% CI, -4.5% to 12.6%]).
Conclusions and relevance: This systematic review and meta-analysis of observational studies found that among patients undergoing radical hysterectomy for early-stage cervical cancer, minimally invasive radical hysterectomy was associated with an elevated risk of recurrence and death compared with open surgery.
Conflict of interest statement
Figures
Comment in
-
Minimally Invasive Surgery for Gynecologic Cancers-A Cautionary Tale.JAMA Oncol. 2020 Jul 1;6(7):991-993. doi: 10.1001/jamaoncol.2020.1617. JAMA Oncol. 2020. PMID: 32525507 No abstract available.
References
-
- Sedlis A, Bundy BN, Rotman MZ, Lentz SS, Muderspach LI, Zaino RJ. A randomized trial of pelvic radiation therapy versus no further therapy in selected patients with stage IB carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy: a Gynecologic Oncology Group study. Gynecol Oncol. 1999;73(2):177-183. doi:10.1006/gyno.1999.5387 - DOI - PubMed
-
- Peters WA III, Liu PY, Barrett RJ II, et al. . Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix. J Clin Oncol. 2000;18(8):1606-1613. doi:10.1200/JCO.2000.18.8.1606 - DOI - PubMed
-
- Clark JG. A more radical method of performing hysterectomy for cancer of the uterus. Bull Johns Hopkins Hosp. 1895;6:120-124.
-
- Ries E. The operative treatment of cancer of the cervix. JAMA. 1906;XLVII(23):1869-1872. doi:10.1001/jama.1906.25210230005001b - DOI
