

Association of Weight-Adjusted Caffeine and β-Blocker Use With Ophthalmology Fellow Performance During Simulated Vitreoretinal Microsurgery
- PMID: 32525517
- PMCID: PMC7290718
- DOI: 10.1001/jamaophthalmol.2020.1971
Association of Weight-Adjusted Caffeine and β-Blocker Use With Ophthalmology Fellow Performance During Simulated Vitreoretinal Microsurgery
Abstract
Importance: Vitreoretinal surgery can be technically challenging and is limited by physiologic characteristics of the surgeon. Factors that improve accuracy and precision of the vitreoretinal surgeon are invaluable to surgical performance.
Objectives: To establish weight-adjusted cutoffs for caffeine and β-blocker (propranolol) intake and to determine their interactions in association with the performance of novice vitreoretinal microsurgeons.
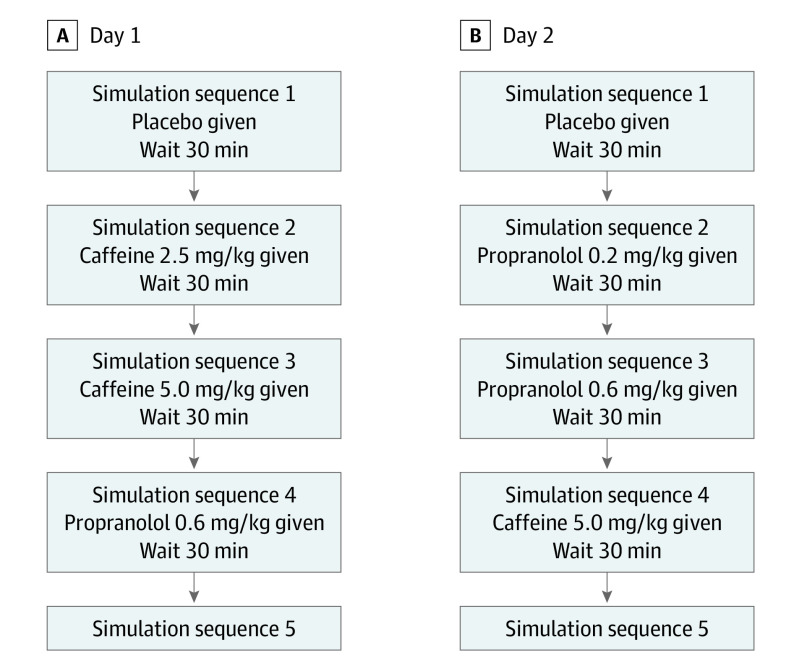
Design, settings, and participants: This single-blind cross-sectional study of 15 vitreoretinal surgeons who had less than 2 years of surgical experience was conducted from September 19, 2018, to September 25, 2019, at a dry-laboratory setting. Five simulations were performed daily for 2 days. On day 1, performance was assessed after sequential exposure to placebo, low-dose caffeine (2.5 mg/kg), high-dose caffeine (5.0 mg/kg), and high-dose propranolol (0.6 mg/kg). On day 2, performance was assessed after sequential exposure to placebo, low-dose propranolol (0.2 mg/kg), high-dose propranolol (0.6 mg/kg), and high-dose caffeine (5.0 mg/kg).
Interventions: Surgical simulation tasks were repeated 30 minutes after masked ingestion of placebo, caffeine, or propranolol pills during the 2 days.
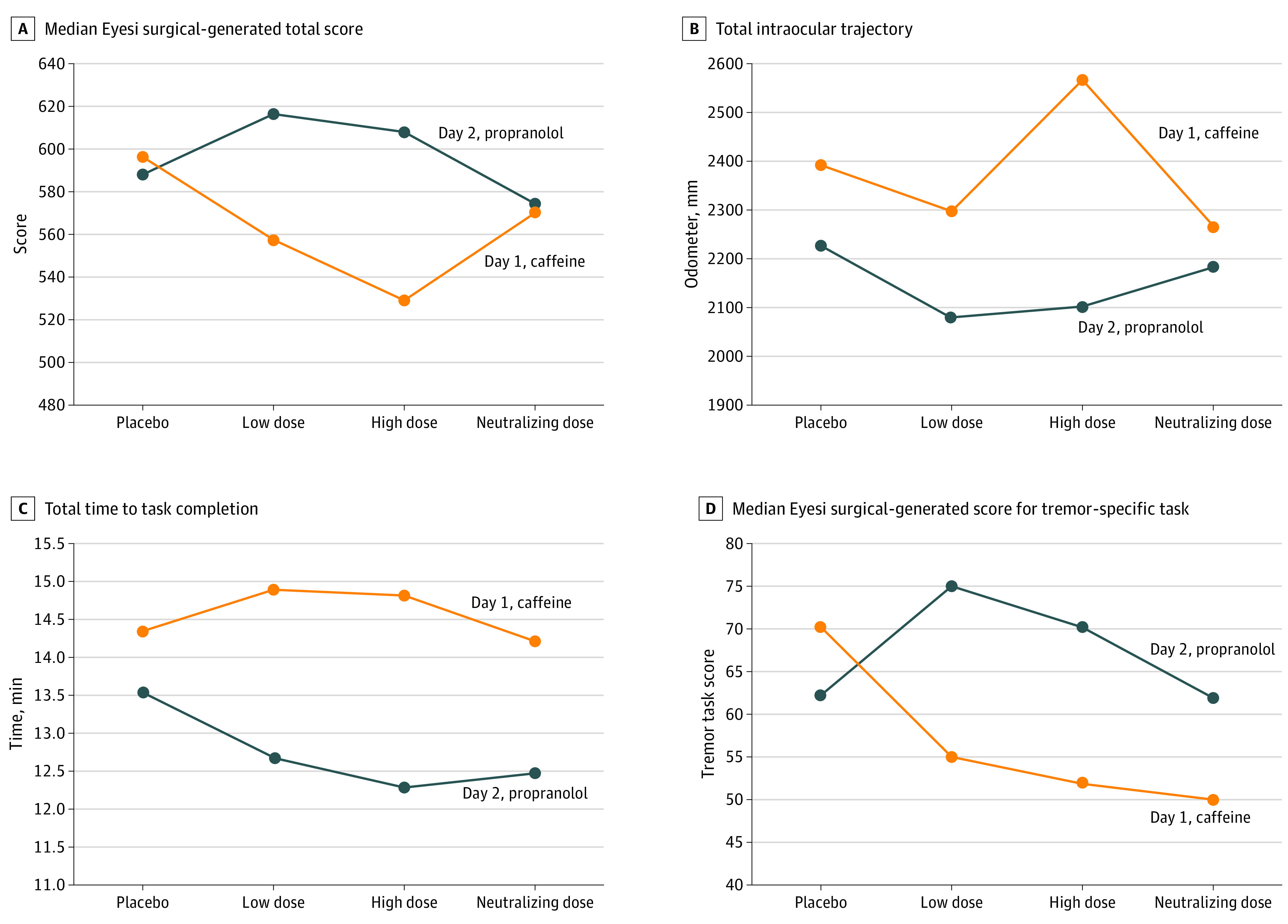
Main outcomes and measures: An Eyesi surgical simulator was used to assess surgical performance, which included surgical score (range, 0 [worst] to 700 [best]), task completion time, intraocular trajectory, and tremor rate (range, 0 [worst] to 100 [best]). The nonparametric Friedman test followed by Dunn-Bonferroni post hoc test was applied for multiple comparisons.
Results: Of 15 vitreoretinal surgeons, 9 (60%) were male, with a mean (SD) age of 29.6 (1.4) years and mean (SD) body mass index (calculated as weight in kilograms divided by height in meters squared) of 23.15 (2.9). Compared with low-dose propranolol, low-dose caffeine was associated with a worse total surgical score (557.0 vs 617.0; difference, -53.0; 95% CI, -99.3 to -6.7; P = .009), a lower antitremor maneuver score (55.0 vs 75.0; difference, -12.0; 95% CI, -21.2 to -2.8; P = .009), longer intraocular trajectory (2298.6 vs 2080.7 mm; difference, 179.3 mm; 95% CI, 1.2-357.3 mm; P = .048), and increased task completion time (14.9 minutes vs 12.7 minutes; difference, 2.3 minutes; 95% CI, 0.8-3.8 minutes; P = .048). Postcaffeine treatment with propranolol was associated with performance improvement; however, surgical performance remained inferior compared with low-dose propranolol alone for total surgical score (570.0 vs 617.0; difference, -51.0; 95% CI, -77.6 to -24.4; P = .01), tremor-specific score (50.0 vs 75.0; difference, -16.0; 95% CI, -31.8 to -0.2; P = .03), and intraocular trajectory (2265.9 mm vs 2080.7 mm; difference, 166.8 mm; 95% CI, 64.1-269.6 mm; P = .03).
Conclusions and relevance: The findings suggest that performance of novice vitreoretinal surgeons was worse after receiving low-dose caffeine alone but improved after receiving low-dose propranolol alone. Their performance after receiving propranolol alone was better than after the combination of propranolol and caffeine. These results may be helpful for novice vitreoretinal surgeons to improve microsurgical performance.
Conflict of interest statement
Figures
Comment in
-
Studies of Microsurgical Skill-The Key Lies in the Design.JAMA Ophthalmol. 2021 Jan 1;139(1):127. doi: 10.1001/jamaophthalmol.2020.4755. JAMA Ophthalmol. 2021. PMID: 33151277 No abstract available.
-
Studies of Microsurgical Skill-The Key Lies in the Design-Reply.JAMA Ophthalmol. 2021 Jan 1;139(1):127-128. doi: 10.1001/jamaophthalmol.2020.4758. JAMA Ophthalmol. 2021. PMID: 33151292 No abstract available.
References
-
- Vander Poorten E, Esteveny L, Gijbels A, et al. Use case for European robotics in ophthalmologic micro-surgery. In: Proceedings of the Fifth Joint Workshop on New Technologies for Computer/Robot Assisted Surgery; 2015:10-12.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
