

Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: a two-centre descriptive study
- PMID: 32526193
- PMCID: PMC7279758
- DOI: 10.1016/S1473-3099(20)30434-5
Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: a two-centre descriptive study
Abstract
Background: COVID-19 is characterised by respiratory symptoms, which deteriorate into respiratory failure in a substantial proportion of cases, requiring intensive care in up to a third of patients admitted to hospital. Analysis of the pathological features in the lung tissues of patients who have died with COVID-19 could help us to understand the disease pathogenesis and clinical outcomes.
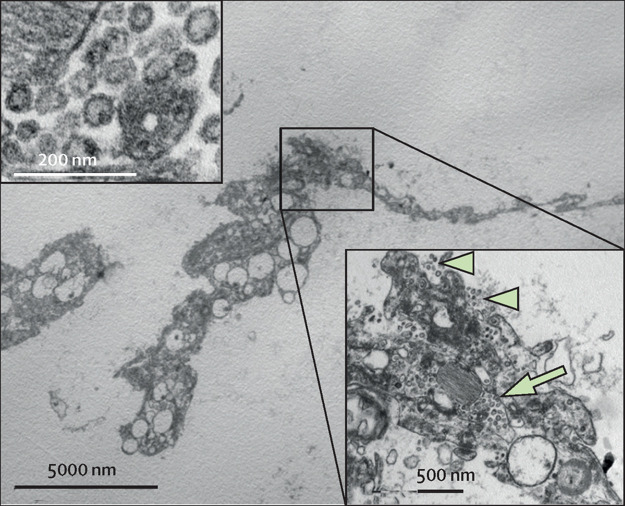
Methods: We systematically analysed lung tissue samples from 38 patients who died from COVID-19 in two hospitals in northern Italy between Feb 29 and March 24, 2020. The most representative areas identified at macroscopic examination were selected, and tissue blocks (median seven, range five to nine) were taken from each lung and fixed in 10% buffered formalin for at least 48 h. Tissues were assessed with use of haematoxylin and eosin staining, immunohistochemical staining for inflammatory infiltrate and cellular components (including staining with antibodies against CD68, CD3, CD45, CD61, TTF1, p40, and Ki-67), and electron microscopy to identify virion localisation.
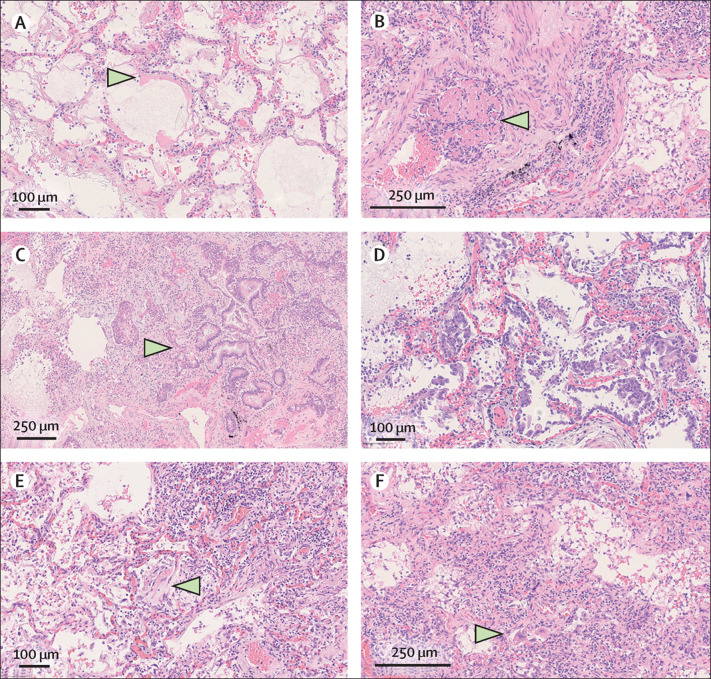
Findings: All cases showed features of the exudative and proliferative phases of diffuse alveolar damage, which included capillary congestion (in all cases), necrosis of pneumocytes (in all cases), hyaline membranes (in 33 cases), interstitial and intra-alveolar oedema (in 37 cases), type 2 pneumocyte hyperplasia (in all cases), squamous metaplasia with atypia (in 21 cases), and platelet-fibrin thrombi (in 33 cases). The inflammatory infiltrate, observed in all cases, was largely composed of macrophages in the alveolar lumina (in 24 cases) and lymphocytes in the interstitium (in 31 cases). Electron microscopy revealed that viral particles were predominantly located in the pneumocytes.
Interpretation: The predominant pattern of lung lesions in patients with COVID-19 patients is diffuse alveolar damage, as described in patients infected with severe acute respiratory syndrome and Middle East respiratory syndrome coronaviruses. Hyaline membrane formation and pneumocyte atypical hyperplasia are frequent. Importantly, the presence of platelet-fibrin thrombi in small arterial vessels is consistent with coagulopathy, which appears to be common in patients with COVID-19 and should be one of the main targets of therapy.
Funding: None.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Pathologists in pursuit of the COVID-19 culprit.Lancet Infect Dis. 2020 Oct;20(10):1102-1103. doi: 10.1016/S1473-3099(20)30449-7. Epub 2020 Jun 8. Lancet Infect Dis. 2020. PMID: 32526191 Free PMC article. No abstract available.
-
Lung fibrosis: an undervalued finding in COVID-19 pathological series.Lancet Infect Dis. 2021 Apr;21(4):e72. doi: 10.1016/S1473-3099(20)30582-X. Epub 2020 Jul 28. Lancet Infect Dis. 2021. PMID: 32735785 Free PMC article. No abstract available.
-
The pathogenesis of thromboembolic disease in covid-19 patients: Could be a catastrophic antiphospholipid syndrome?Thromb Res. 2020 Oct;194:192-194. doi: 10.1016/j.thromres.2020.06.042. Epub 2020 Jun 27. Thromb Res. 2020. PMID: 32788116 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
