

Urinary Lithogenic Risk Profile in ADPKD Patients Treated with Tolvaptan
- PMID: 32527945
- PMCID: PMC7341771
- DOI: 10.2215/CJN.13861119
Urinary Lithogenic Risk Profile in ADPKD Patients Treated with Tolvaptan
Abstract
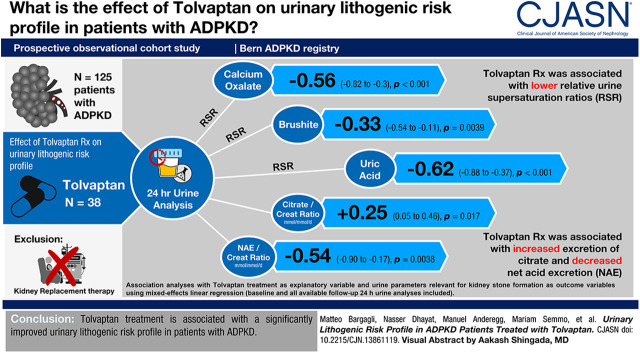
Background and objectives: Nephrolithiasis is a common health problem in autosomal dominant polycystic kidney disease (ADPKD) and significantly contributes to patient morbidity. Recently, Tolvaptan has been introduced for the treatment of ADPKD, but whether it is associated with alterations of the urinary lithogenic risk profile remains unknown.
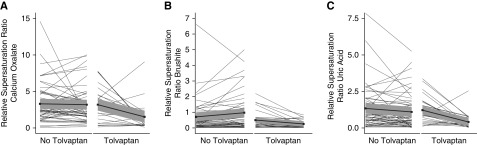
Design, setting, participants, & measurements: We conducted an analysis of participants enrolled in the Bern ADPKD registry, a prospective observational cohort study. Twenty-four-hour urine analyses were performed at baseline and then at yearly follow-ups. Relative supersaturation ratios for calcium oxalate, brushite, and uric acid were calculated with the program EQUIL2. Unadjusted and multivariable mixed-effects linear regression models, adjusted for age, sex, body mass index, eGFR, net acid excretion, and height-adjusted total kidney volume, were used to assess the association of Tolvaptan with urinary parameters relevant for kidney stone formation. The maximum individual follow-up time was 3 years, median follow-up time 1.9 years, and cumulative follow-up time 169 years.
Results: In total, 125 participants (38 with and 87 without Tolvaptan treatment) were included in the analysis. In multivariable analysis, Tolvaptan treatment was associated [adjusted estimate of the difference between Tolvaptan and no Tolvaptan; 95% confidence interval (CI)] with lower urine relative supersaturation ratios for calcium oxalate (-0.56; 95% CI, -0.82 to -0.3; P<0.001), brushite (-0.33; 95% CI, -0.54 to -0.11; P=0.004), and uric acid (-0.62; 95% CI, -0.88 to -0.37; P<0.001), and with higher urine citrate in mmol/mmol creatinine per day (0.25; 95% CI, 0.05 to 0.46; P=0.02) and calcium in mmol/mmol creatinine per day (0.31; 95% CI, 0.09 to 0.53; P=0.006) excretion. In addition, Tolvaptan treatment was associated with lower net acid excretion in mEq/mmol creatinine per day (-0.54; 95% CI, -0.90 to -0.17; P=0.004) and higher net gastrointestinal alkali absorption in mEq/mmol creatinine per day (0.57; 95% CI, 0.26 to 0.88; P<0.001).
Conclusions: Tolvaptan treatment is associated with a significantly improved urinary lithogenic risk profile in patients with ADPKD.
Keywords: ADPKD; alkalies; autosomal dominant; body mass index; calcium oxalate; calcium phosphate; citric acid; cohort studies; creatinine; dibasic; dihydrate; follow-up studies; glomerular filtration rate; kidney calculi; kidney stones; linear models; polycystic kidney; prospective studies; tolvaptan; uric acid.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
ADPKD, Tolvaptan, and Nephrolithiasis Risk.Clin J Am Soc Nephrol. 2020 Jul 1;15(7):923-925. doi: 10.2215/CJN.07610520. Epub 2020 Jun 11. Clin J Am Soc Nephrol. 2020. PMID: 32527947 Free PMC article. No abstract available.
-
Re: Urinary Lithogenic Risk Profile in ADPKD Patients Treated with Tolvaptan.J Urol. 2020 Nov;204(5):1090-1091. doi: 10.1097/JU.0000000000001258.01. Epub 2020 Aug 21. J Urol. 2020. PMID: 32820999 No abstract available.
References
-
- Kramer A, Pippias M, Noordzij M, Stel VS, Andrusev AM, Aparicio-Madre MI, Arribas Monzón FE, Åsberg A, Barbullushi M, Beltrán P, Bonthuis M, Caskey FJ, Castro de la Nuez P, Cernevskis H, De Meester J, Finne P, Golan E, Heaf JG, Hemmelder MH, Ioannou K, Kantaria N, Komissarov K, Korejwo G, Kramar R, Lassalle M, Lopot F, Macário F, Mackinnon B, Pálsson R, Pechter Ü, Piñera VC, Santiuste de Pablos C, Segarra-Medrano A, Seyahi N, Slon Roblero MF, Stojceva-Taneva O, Vazelov E, Winzeler R, Ziginskiene E, Massy Z, Jager KJ: The European renal association - European dialysis and transplant association (ERA-EDTA) registry annual report 2016: A summary. Clin Kidney J 12: 702–720, 2019. - PMC - PubMed
-
- Porath B, Gainullin VG, Cornec-Le Gall E, Dillinger EK, Heyer CM, Hopp K, Edwards ME, Madsen CD, Mauritz SR, Banks CJ, Baheti S, Reddy B, Herrero JI, Bañales JM, Hogan MC, Tasic V, Watnick TJ, Chapman AB, Vigneau C, Lavainne F, Audrézet M-P, Ferec C, Le Meur Y, Torres VE, Harris PC; Genkyst Study Group, HALT Progression of Polycystic Kidney Disease Group; Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease : Mutations in GANAB, encoding the glucosidase IIα subunit, cause autosomal-dominant polycystic kidney and liver disease. Am J Hum Genet 98: 1193–1207, 2016. - PMC - PubMed
-
- Chapman AB, Devuyst O, Eckardt K-U, Gansevoort RT, Harris T, Horie S, Kasiske BL, Odland D, Pei Y, Perrone RD, Pirson Y, Schrier RW, Torra R, Torres VE, Watnick T, Wheeler DC; Conference Participants : Autosomal-dominant polycystic kidney disease (ADPKD): Executive summary from a kidney disease: Improving global outcomes (KDIGO) controversies conference. Kidney Int 88: 17–27, 2015. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
