

A Comparison of Hip Spica Casting to Short Leg Casts and Bar after Hip Reconstruction in Cerebral Palsy
- PMID: 32528767
- PMCID: PMC7282370
- DOI: 10.7759/cureus.8028
A Comparison of Hip Spica Casting to Short Leg Casts and Bar after Hip Reconstruction in Cerebral Palsy
Abstract
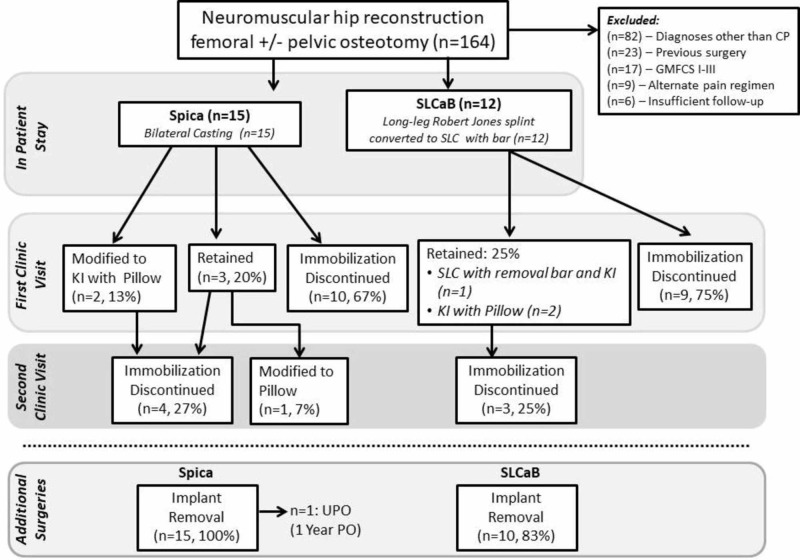
Background Immobilization after hip reconstruction in children with cerebral palsy varies according to surgeon preference. The effect of postoperative immobilization on postoperative pain is unknown. Success in achieving hip stability and complications may also differ depending on the immobilization technique utilized. Questions/purposes Using retrospective data, we aimed to evaluate: (a) what effect does postoperative immobilization with hip spica casting versus short leg casts and bar (SLCaB); have on pain and pain management in children with quadriplegic cerebral palsy undergoing femoral and/or pelvic osteotomy? and (b) Do complications and radiographic outcomes differ between those treated postoperatively with hip spica casting and those in short leg casts? Materials and Methods Children with quadriplegic cerebral palsy (GMFCS IV-V, mean age 7.8 years [range: 3-15 years]) undergoing femoral or pelvic osteotomy between 2012 and 2014 in the treatment of spastic hip subluxation were reviewed. Modes of immobilization were compared, between spica casting (n=15) and SLCaB (n=12). Preoperative, perioperative, and postoperative pain was quantified between groups. In-hospital epidural dosage, morphine equivalent dosages (MED), adjunctive medications, early maintenance of radiographic hip stability, and all complications were noted and analyzed. Results Children were more likely to have spica cast immobilization if they were younger. Postoperative pain scores were similar between groups, with comparable patterns of epidural and MED administered during hospitalization. Spica casts were often flared up during hospitalization, but skin ulcers were uncommon and comparable between the two groups. Within 12 months of surgery, more ipsilateral femur fractures were observed distant to implants in the hip spica group, although the incidence of fractures did not meet statistical thresholds. Conclusion Spica casting and SLCaB after neuromuscular hip reconstruction did not show a difference in hip stability, narcotic pain medication usage or complication profile.
Keywords: cerebral palsy; neuromuscular hip subluxation; spastic hip subluxation; spica cast.
Copyright © 2020, Truong et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Combined hip surgery in cerebral palsy patients. Atar D, Grant AD, Bash J, Lehman WB. https://www.ncbi.nlm.nih.gov/pubmed/7773656. Am J Orthop (Belle Mead NJ) 1995;24:52–55. - PubMed
-
- Clinical benefit of reconstruction of dislocated or subluxated hip joints in patients with spastic cerebral palsy. Brunner R, Baumann JU. J Pediatr Orthop. 1994;14:290–294. - PubMed
-
- Pemberton pelvic osteotomy and varus rotational osteotomy in the treatment of acetabular dysplasia in patients who have static encephalopathy. Gordon JE, Capelli AM, Strecker WB, Delgado ED, Schoenecker PL. J Bone Joint Surg Am. 1996;78:1863–1871. - PubMed
-
- One-stage correction of the dysplastic hip in cerebral palsy with the San Diego acetabuloplasty: results and complications in 104 hips. McNerney NP, Mubarak SJ, Wenger DR. https://journals.lww.com/pedorthopaedics/Fulltext/2000/01000/One_Stage_C.... J Pediatr Orthop. 2000;20:93–103. - PubMed
-
- One-stage correction of the spastic dislocated hip. Use of pericapsular acetabuloplasty to improve coverage. Mubarak SJ, Valencia FG, Wenger DR. https://journals.lww.com/jbjsjournal/Abstract/1992/74090/One_stage_corre.... J Bone Joint Surg Am. 1992;74:1347–1357. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous