

Metastatic Melanoma Epidural Tumour Regression Following Percutaneous Radiofrequency Ablation
- PMID: 32528775
- PMCID: PMC7282353
- DOI: 10.7759/cureus.8039
Metastatic Melanoma Epidural Tumour Regression Following Percutaneous Radiofrequency Ablation
Abstract
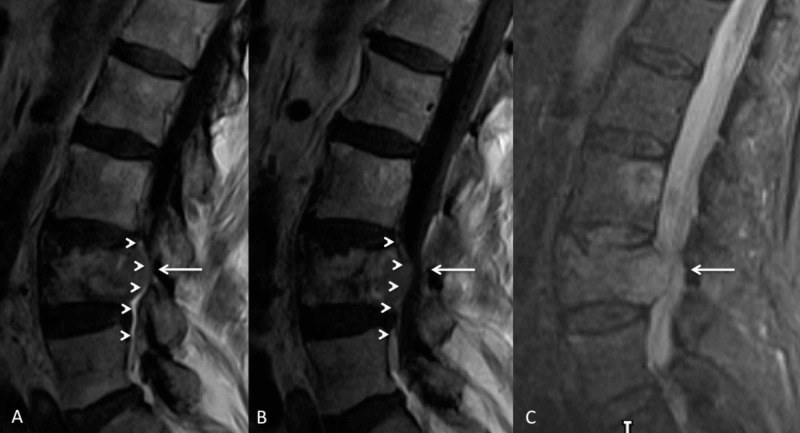
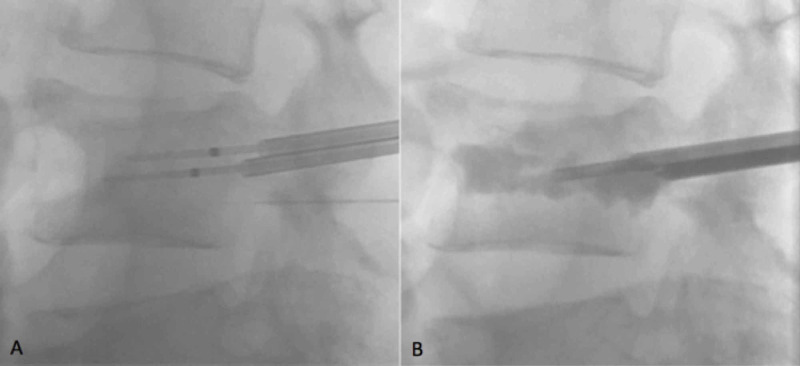
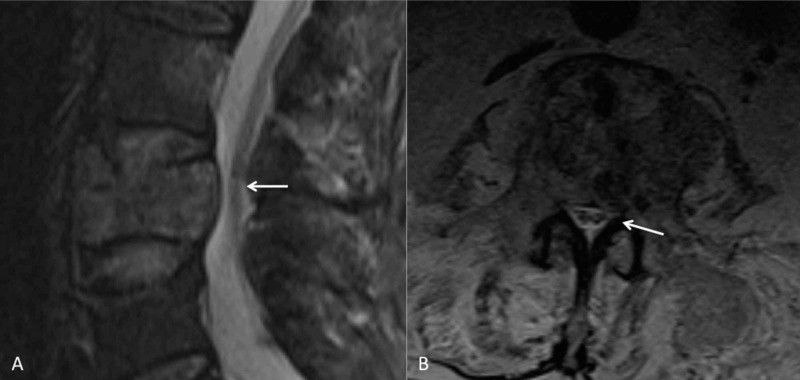
Percutaneous radiofrequency ablation of spinal metastases is an emerging treatment for patients with painful metastatic spine disease. It is typically performed for patients who have not responded to conventional treatments or who have contraindications to radiotherapy. Destruction of the posterior wall of the vertebral body and epidural disease may be considered relative contraindications for radiofrequency ablation. This is due to the difficulty in achieving satisfactory ablation balanced against the risk of neural injury. We describe a case of metastatic melanoma with an expansile lytic metastasis and epidural tumour extension at the L4 vertebral body level resulting in severe central canal stenosis. This was successfully treated with percutaneous radiofrequency ablation and vertebral augmentation. The patient reported significant pain relief post-procedure and follow-up MRI at two months demonstrated local tumour regression, epidural disease resolution and improved spinal canal dimensions. To the best of our knowledge, this is the first report of epidural disease resolution from metastatic melanoma following radiofrequency ablation and emphasises the potential benefits of ablation therapy even in the presence of canal stenosis and epidural metastatic disease.
Keywords: back pain; bone metastases; interventional radiology; malignant melanoma metastasis; musculoskeletal radiology; radiofrequency ablation; spinal metastases.
Copyright © 2020, Papanikitas et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- A systematic review of evidence on malignant spinal metastases: natural history and technologies for identifying patients at high risk of vertebral fracture and spinal cord compression. Sutcliffe P, Connock M, Shyangdan D, Court R, Kandala N-B, Clarke A. Health Technol Assess. 2013;17:1–274. - PMC - PubMed
-
- Spine metastases: current treatments and future directions. Harel R, Angelov L. Eur J Cancer. 2010;46:2696–2707. - PubMed
-
- Percutaneous spinal ablation in a sheep model: protective capacity of an intact cortex, correlation of ablation parameters with ablation zone size, and correlation of postablation MRI and pathologic findings. Wallace AN, Hillen TJ, Friedman MV, et al. AJNR Am J Neuroradiol. 2017;38:1653–1659. - PMC - PubMed
-
- Lower extremity paralysis after radiofrequency ablation of vertebral metastases. Huntoon K, Eltobgy M, Mohyeldin A, Elder JB. World Neurosurg. 2020;133:178–184. - PubMed
Publication types
LinkOut - more resources
Full Text Sources