

Primary Cutaneous B-Cell Lymphomas: An Update
- PMID: 32528871
- PMCID: PMC7266949
- DOI: 10.3389/fonc.2020.00651
Primary Cutaneous B-Cell Lymphomas: An Update
Abstract
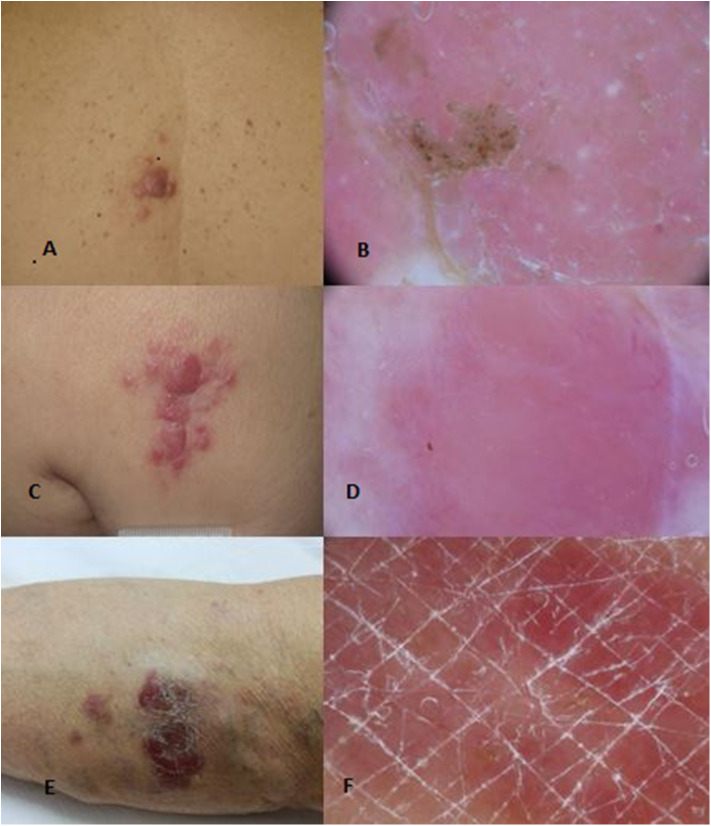
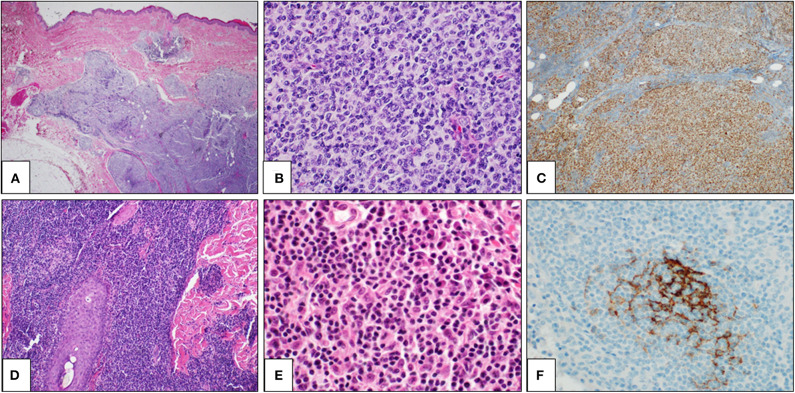
Primary cutaneous B-cell lymphomas (PCBCLs) comprise a group of extranodal B-cell non-Hodgkin lymphomas B-cell derived, which primarily involve the skin without evidence of extracutaneous disease at the time of diagnosis. They include ~25% of all cutaneous lymphomas and are classified in three major subgroups (World Health Organization (WHO) 2017): primary cutaneous marginal zone lymphoma (PCMZL), primary cutaneous follicle-center cell lymphoma (PCFCL), and diffuse large B-cell lymphoma, leg type (PCDLBCL, LT). This classification also includes some less common entities such as intravascular large B-cell lymphoma. Recently, WHO-EORTC added Epstein-Barr virus positive (EBV+) mucocutaneous ulcer, as a new provisional distinct entity, to cutaneous B-cell lymphomas. PCBCLs are classically characterized by patches, plaques, or nodules showing great variability for color, shape, and location. Diagnosis requires histological examination with immunohistochemical staining. In general, therapeutic options depend on the exact histological and immunohistochemical classification, disease presentation, and risk assessment. PCMZL and PCFCL are considered indolent lymphomas with a good prognosis and are associated with 5-year disease-specific survival ≥ 95%. In contrast, PCDLBCL, LT is considered an aggressive lymphoma with a survival rate in 5 years of lower than 60%. Patients with a solitary lesion or limited lesions in a single anatomical site require different treatments as compared to patients with generalized lesions or refractory disease or extracutaneous involvement. Therapeutic choice includes observation, local, or systemic therapy based on histology and disease extension. Patient management is multidisciplinary, including dermatologists, pathologists, hemato-oncologists, and radiation oncologists.
Keywords: EBV-positive mucocutaneous ulcer; diffuse large B-cell lymphoma; intravascular large B-cell lymphoma; leg type; primary cutaneous follicle-center cell lymphoma; primary cutaneous marginal zone lymphoma.
Copyright © 2020 Vitiello, Sica, Ronchi, Caccavale, Franco and Argenziano.
Figures
References
-
- WHO Classification of Tumours of Haematopoietic and Lymphoid Tissue. Lyon: IARC; (2008).
Publication types
LinkOut - more resources
Full Text Sources