

Prevalence and Persistence of Uremic Symptoms in Incident Dialysis Patients
- PMID: 32529191
- PMCID: PMC7289028
- DOI: 10.34067/kid.0000072019
Prevalence and Persistence of Uremic Symptoms in Incident Dialysis Patients
Abstract
Background: Uremic symptoms are major contributors to the poor quality of life among patients on dialysis, but whether their prevalence or intensity has changed over time is unknown.
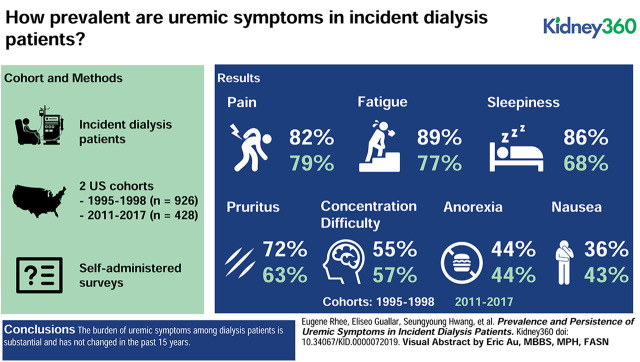
Methods: We examined responses to validated questionnaires in two incident dialysis cohort studies, the Choices for Health Outcomes in Caring for ESRD (CHOICE) study (N=926, 1995-1998) and the Longitudinal United States/Canada Incident Dialysis (LUCID) study (N=428, 2011-2017). We determined the prevalence and severity of uremic symptoms-anorexia, nausea/vomiting, pruritus, sleepiness, difficulty concentrating, fatigue, and pain-in both cohorts.
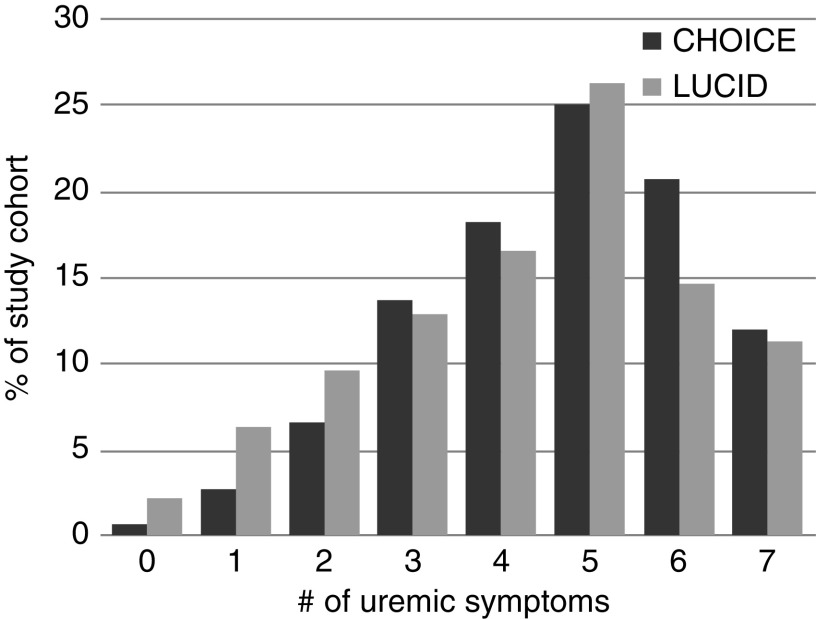
Results: In CHOICE and LUCID, respectively, mean age of the participants was 58 and 60 years, 53% and 60% were male, and 28% and 32% were black. In both cohorts, 54% of the participants had diabetes. Median time from dialysis initiation to the symptoms questionnaires was 45 days for CHOICE and 77 days for LUCID. Uremic symptom prevalence in CHOICE did not change from baseline to 1-year follow-up and was similar across CHOICE and LUCID. Baseline symptom prevalence in CHOICE and LUCID was as follows: anorexia (44%, 44%, respectively), nausea/vomiting (36%, 43%), pruritus (72%, 63%), sleepiness (86%, 68%), difficulty concentrating (55%, 57%), fatigue (89%, 77%), and pain (82%, 79%). In both cohorts, >80% of patients had three or more symptoms and >50% had five or more symptoms. The correlation between individual symptoms was low (ρ<0.5 for all comparisons). In CHOICE, no clinical or laboratory parameter was strongly associated with multiple symptoms.
Conclusions: The burden of uremic symptoms among patients on dialysis is substantial and has not changed in the past 15 years. Improving quality of life will require identification of the factors that underlie the pathogenesis of uremic symptoms and better ways of removing the toxins that are responsible.
Conflict of interest statement
E. Guallar reports grants from the National Institutes of Health (NIH) during the conduct of the study. S. Moe reports personal fees from Amgen, personal fees from Ardelyx, grants from Chugai, grants from Keryx/Akebia, grants from the NIH, and grants from Veterans Administration, outside the submitted work. T. Shafi reports grants from the NIH during the conduct of the study and personal fees from Siemens outside the submitted work. R. Thadhani reports personal fees from Fresenius Medical Care during the conduct of the study. M. Tonelli reports an honorarium from B Braun that was donated to charity and grants from the Canadian Institutes of Health Research during the conduct of the study. J. Himmelfarb, S. Hwang, N. Kim, N. Powe, and E. Rhee have nothing to disclose.
Figures
References
-
- Saran R, Li Y, Robinson B, Ayanian J, Balkrishnan R, Bragg-Gresham J, Chen JT, Cope E, Gipson D, He K, Herman W, Heung M, Hirth RA, Jacobsen SS, Kalantar-Zadeh K, Kovesdy CP, Leichtman AB, Lu Y, Molnar MZ, Morgenstern H, Nallamothu B, O’Hare AM, Pisoni R, Plattner B, Port FK, Rao P, Rhee CM, Schaubel DE, Selewski DT, Shahinian V, Sim JJ, Song P, Streja E, Kurella Tamura M, Tentori F, Eggers PW, Agodoa LY, Abbott KC: US renal data system 2014 annual data report: Epidemiology of kidney disease in the United States. Am J Kidney Dis 66[Suppl 1]: S1–S305, 2015 - PMC - PubMed
-
- Ramkumar N, Beddhu S, Eggers P, Pappas LM, Cheung AK: Patient preferences for in-center intense hemodialysis. Hemodial Int 9: 281–295, 2005 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
