

Exercise and metabolic health: beyond skeletal muscle
- PMID: 32529412
- PMCID: PMC7377236
- DOI: 10.1007/s00125-020-05177-6
Exercise and metabolic health: beyond skeletal muscle
Abstract
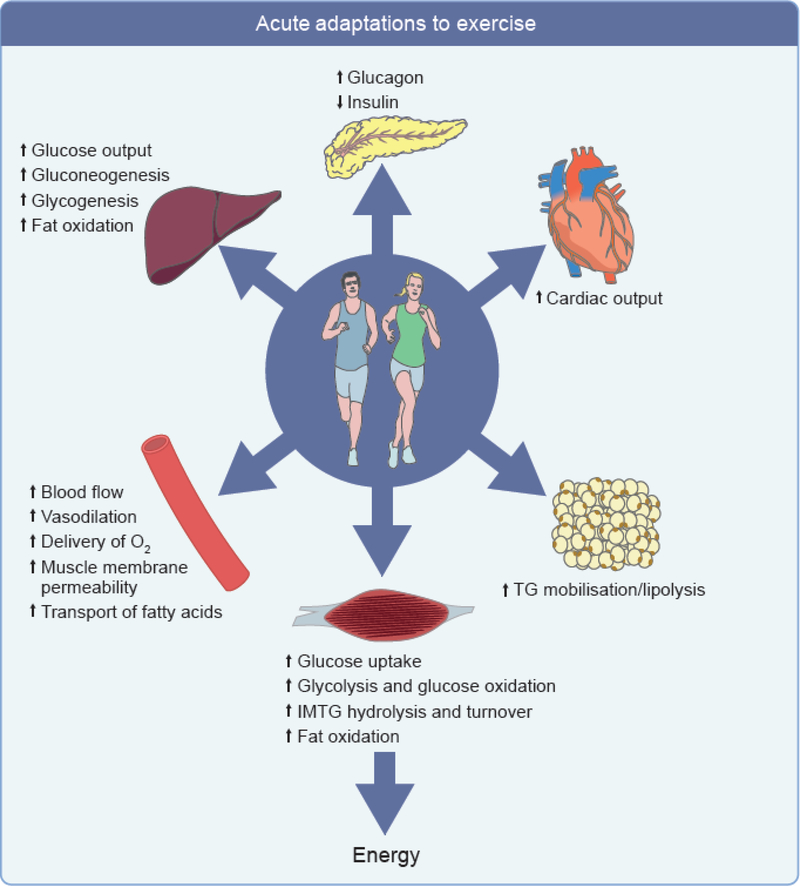
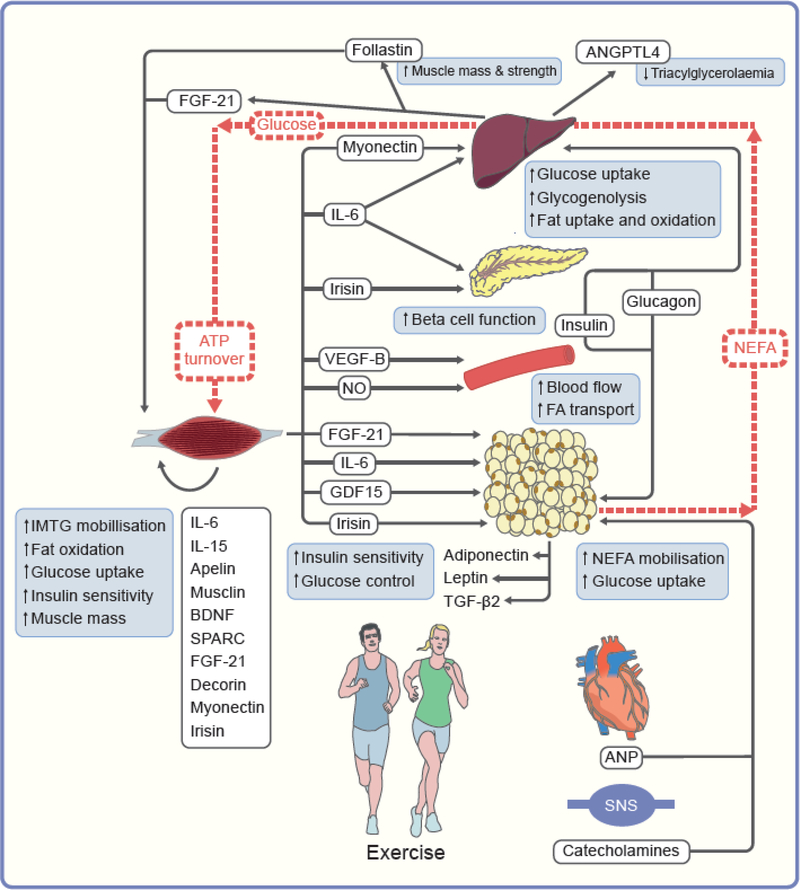
Regular exercise is a formidable regulator of insulin sensitivity and overall systemic metabolism through both acute events driven by each exercise bout and through chronic adaptations. As a result, regular exercise significantly reduces the risks for chronic metabolic disease states, including type 2 diabetes and non-alcoholic fatty liver disease. Many of the metabolic health benefits of exercise depend on skeletal muscle adaptations; however, there is plenty of evidence that exercise exerts many of its metabolic benefit through the liver, adipose tissue, vasculature and pancreas. This review will highlight how exercise reduces metabolic disease risk by activating metabolic changes in non-skeletal-muscle tissues. We provide an overview of exercise-induced adaptations within each tissue and discuss emerging work on the exercise-induced integration of inter-tissue communication by a variety of signalling molecules, hormones and cytokines collectively named 'exerkines'. Overall, the evidence clearly indicates that exercise is a robust modulator of metabolism and a powerful protective agent against metabolic disease, and this is likely to be because it robustly improves metabolic function in multiple organs. Graphical abstract.
Keywords: Adipose tissue; Endothelium; Exercise; Exerkines; Liver; Muscle; NAFLD; Pancreas; Review; Type 2 diabetes.
Figures

References
-
- Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, Smith BK (2009) American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Medicine and science in sports and exercise 41(2): 459–471. 10.1249/MSS.0b013e3181949333 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
