Effect of a Comprehensive Cardiovascular Risk Reduction Intervention in Persons With Serious Mental Illness: A Randomized Clinical Trial
- PMID: 32530472
- PMCID: PMC7293000
- DOI: 10.1001/jamanetworkopen.2020.7247
Effect of a Comprehensive Cardiovascular Risk Reduction Intervention in Persons With Serious Mental Illness: A Randomized Clinical Trial
Abstract
Importance: Persons with serious mental illness have a cardiovascular disease mortality rate more than twice that of the overall population. Meaningful cardiovascular risk reduction requires targeted efforts in this population, who often have psychiatric symptoms and cognitive impairment.
Objective: To determine the effectiveness of an 18-month multifaceted intervention incorporating behavioral counseling, care coordination, and care management for overall cardiovascular risk reduction in adults with serious mental illness.
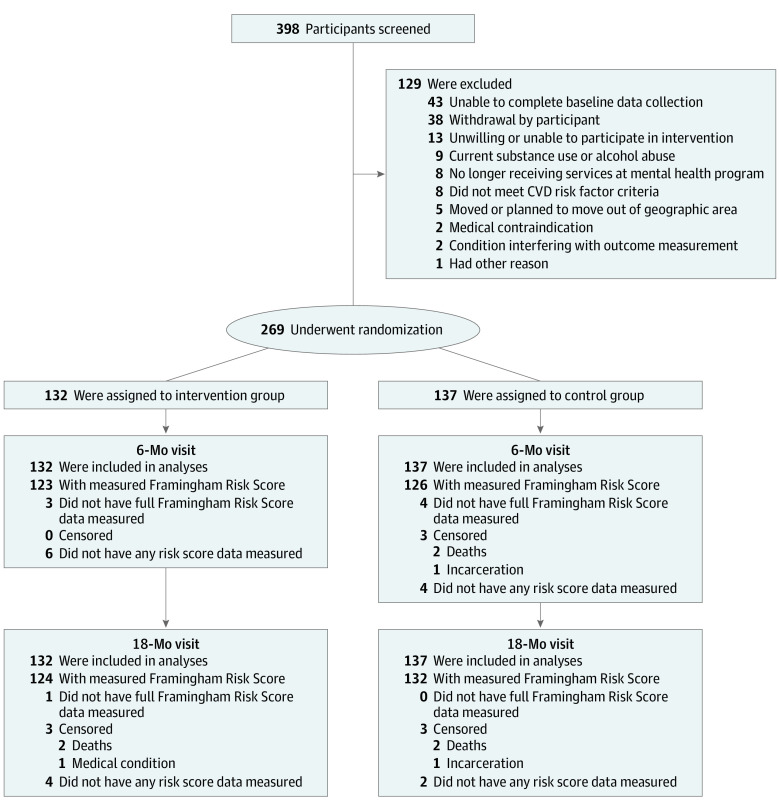
Design, setting, and participants: This randomized clinical trial was conducted from December 2013 to November 2018 at 4 community mental health outpatient programs in Maryland. The study recruited adults with at least 1 cardiovascular disease risk factor (hypertension, diabetes, dyslipidemia, current tobacco smoking, and/or overweight or obesity) attending the mental health programs. Of 398 participants screened, 269 were randomized to intervention (132 participants) or control (137 participants). Data collection staff were blinded to group assignment. Data were analyzed on the principle of intention to treat, and data analysis was performed from November 2018 to March 2019.
Interventions: A health coach and nurse provided individually tailored cardiovascular disease risk reduction behavioral counseling, collaborated with physicians to implement appropriate risk factor management, and coordinated with mental health staff to encourage attainment of health goals. Programs offered physical activity classes and received consultation on serving healthier meals; intervention and control participants were exposed to these environmental changes.
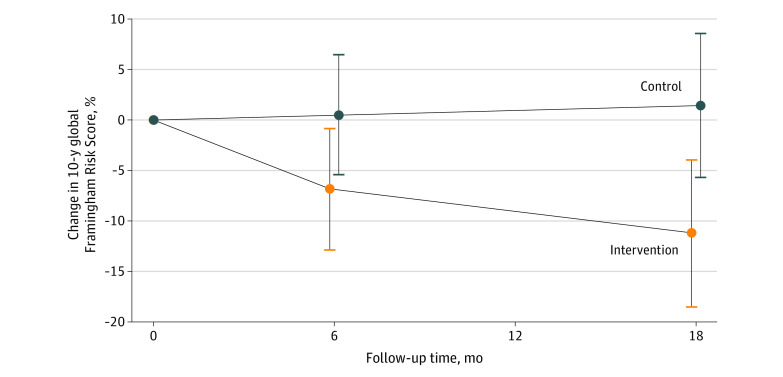
Main outcomes and measures: The primary outcome was the change in the risk of cardiovascular disease from the global Framingham Risk Score (FRS), which estimates the 10-year probability of a cardiovascular disease event, from baseline to 18 months, expressed as percentage change for intervention compared with control.
Results: Of 269 participants randomized (mean [SD] age, 48.8 [11.9] years; 128 men [47.6%]), 159 (59.1%) had a diagnosis of schizophrenia or schizoaffective disorder, 67 (24.9%) had bipolar disorder, and 38 (14.1%) had major depressive disorder. At 18 months, the primary outcome, FRS, was obtained for 256 participants (95.2%). The mean (SD) baseline FRS was 11.5% (11.5%) (median, 8.6%; interquartile range, 3.9%-16.0%) in the intervention group and 12.7% (12.7%) (median, 9.1%; interquartile range, 4.0%-16.7%) in the control group. At 18 months, the mean (SD) FRS was 9.9% (10.2%) (median, 7.7%; interquartile range, 3.1%-12.0%) in the intervention group and 12.3% (12.0%) (median, 9.7%; interquartile range, 4.0%-15.9%) in the control group. Compared with the control group, the intervention group experienced a 12.7% (95% CI, 2.5%-22.9%; P = .02) relative reduction in FRS at 18 months.
Conclusions and relevance: An 18-month behavioral counseling, care coordination, and care management intervention statistically significantly reduced overall cardiovascular disease risk in adults with serious mental illness. This intervention provides the means to substantially reduce health disparities in this high-risk population.
Trial registration: ClinicalTrials.gov Identifier: NCT02127671.
Conflict of interest statement
Figures