

Association of cardiac biomarkers and comorbidities with increased mortality, severity, and cardiac injury in COVID-19 patients: A meta-regression and decision tree analysis
- PMID: 32530509
- PMCID: PMC7307124
- DOI: 10.1002/jmv.26166
Association of cardiac biomarkers and comorbidities with increased mortality, severity, and cardiac injury in COVID-19 patients: A meta-regression and decision tree analysis
Abstract
Background: Coronavirus disease-2019 (COVID-19) has a deleterious effect on several systems, including the cardiovascular system. We aim to systematically explore the association of COVID-19 severity and mortality rate with the history of cardiovascular diseases and/or other comorbidities and cardiac injury laboratory markers.
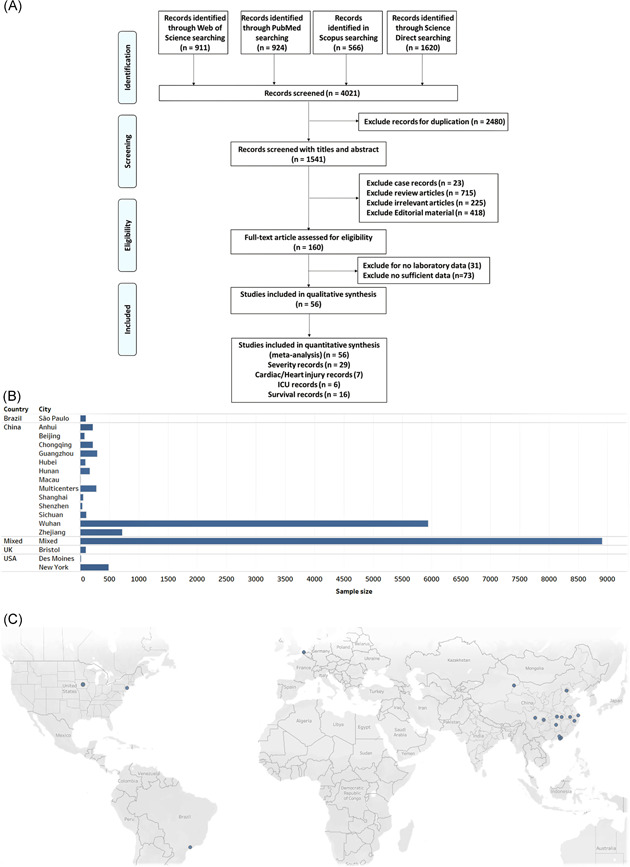
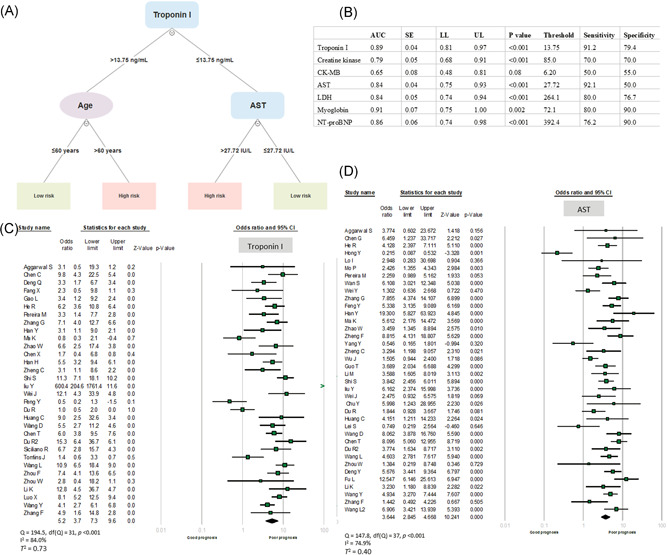
Methods: The standardized mean difference (SMD) or odds ratio (OR) and 95% confidence intervals (CIs) were applied to estimate pooled results from the 56 studies. The prognostic performance of cardiac markers for predicting adverse outcomes and to select the best cutoff threshold was estimated by receiver operating characteristic curve analysis. Decision tree analysis by combining cardiac markers with demographic and clinical features was applied to predict mortality and severity in patients with COVID-19.
Results: A meta-analysis of 17 794 patients showed patients with high cardiac troponin I (OR = 5.22, 95% CI = 3.73-7.31, P < .001) and aspartate aminotransferase (AST) levels (OR = 3.64, 95% CI = 2.84-4.66, P < .001) were more likely to develop adverse outcomes. High troponin I more than 13.75 ng/L combined with either advanced age more than 60 years or elevated AST level more than 27.72 U/L was the best model to predict poor outcomes.
Conclusions: COVID-19 severity and mortality are complicated by myocardial injury. Assessment of cardiac injury biomarkers may improve the identification of those patients at the highest risk and potentially lead to improved therapeutic approaches.
Keywords: COVID-19; SARS-CoV-2; cardiac injury; cardiac markers; meta-analysis; outcome.
© 2020 Wiley Periodicals LLC.
Conflict of interest statement
All the authors declare that there are no conflict of interests.
Figures
References
-
- Ksiazek TG, Erdman D, Goldsmith CS, et al. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med. 2003;348(20):1953‐1966. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
