

Are There Differences in Accuracy or Outcomes Scores Among Navigated, Robotic, Patient-specific Instruments or Standard Cutting Guides in TKA? A Network Meta-analysis
- PMID: 32530896
- PMCID: PMC7431275
- DOI: 10.1097/CORR.0000000000001324
Are There Differences in Accuracy or Outcomes Scores Among Navigated, Robotic, Patient-specific Instruments or Standard Cutting Guides in TKA? A Network Meta-analysis
Abstract
Background: Several kinds of cutting guides, including patient-specific instrumentation, navigation, standard cutting guides, accelerometer-based navigation, and robotic guidance, are available to restore a planned alignment during TKA. No previous study has simultaneously compared all of these devices; a network meta-analysis is an especially appealing method because it allows comparisons across approaches that were not compared head-to-head in individual randomized controlled trials.
Questions/purposes: We performed a network meta-analysis to determine whether novel approaches to achieving implant alignment, such as patient-specific instrumentation, navigation, accelerometer-based navigation, and robotic guidance, provide any advantage over standard cutting guides in terms of: (1) hip-knee-ankle (HKA) alignment outliers greater than ± 3°, (2) outcome scores (1989 - Knee Society Score and WOMAC score) measured 6 months after surgery, or (3) femoral and tibial implant malalignment (greater than ± 3°), taken separately, in the frontal and sagittal plane, as well as other secondary outcomes including validated outcome scores 1 and 2 years after surgery.
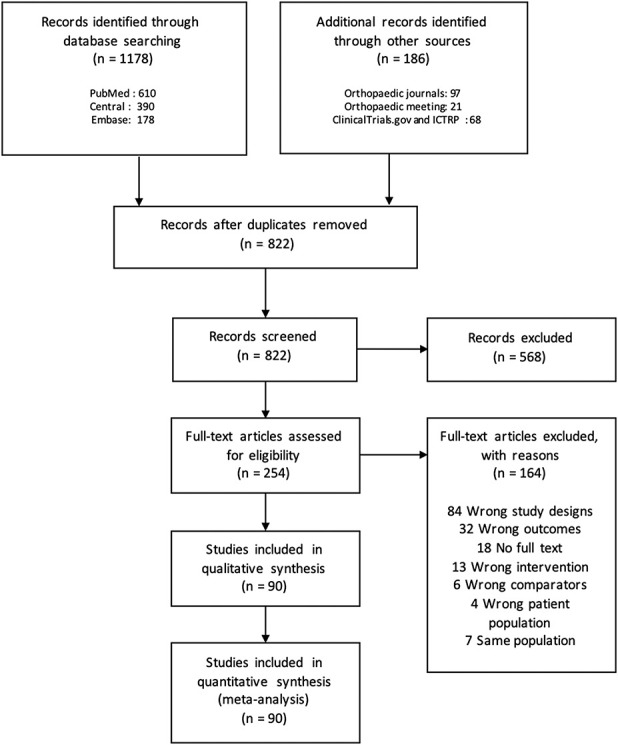
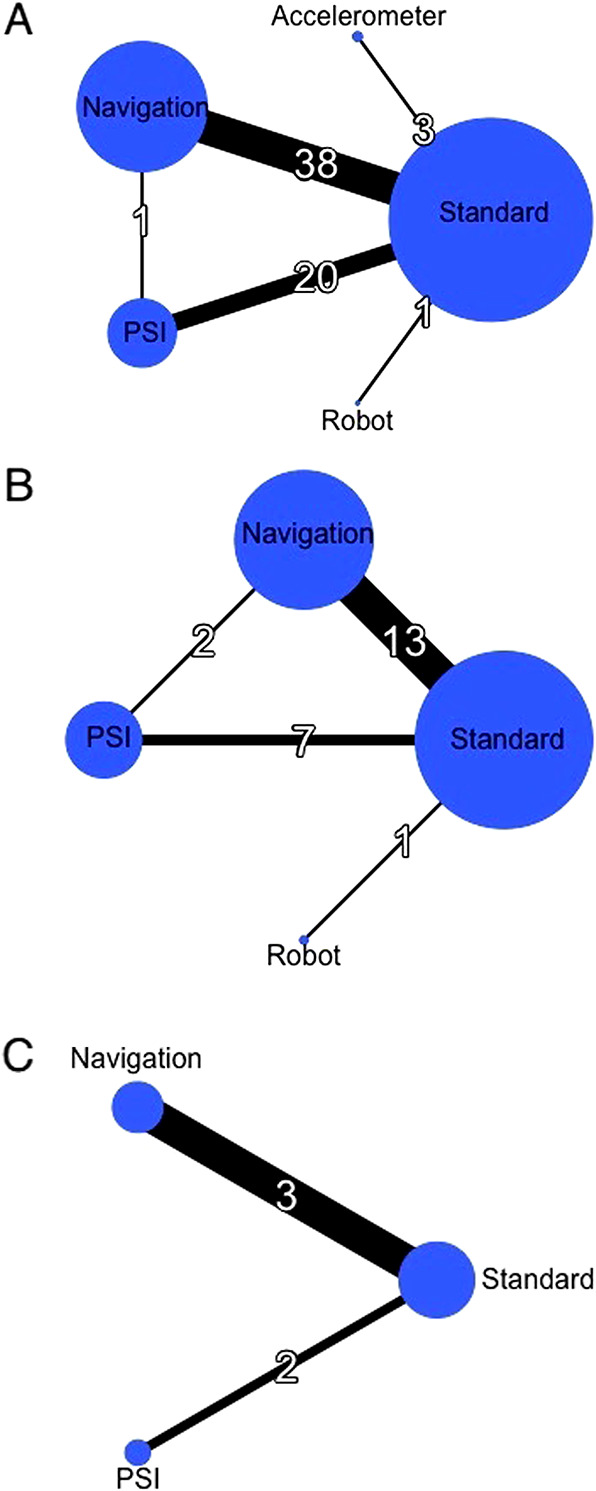
Methods: In our network meta-analysis, we included randomized controlled trials comparing the different cutting guides by using at least one of the previously specified criteria, without limitation on language or date of publication. We searched electronic databases, major orthopaedic journals, proceedings of major orthopaedic meetings, ClinicalTrials.gov, and the World Health Organization's International Clinical Trials Registry Platform until October 1, 2018. This led to the inclusion of 90 randomized controlled trials involving 9389 patients (mean age 68.8 years) with 10,336 TKAs. Two reviewers independently selected trials and extracted data. The primary outcomes were the proportion patients with malalignment of the HKA angle (defined as HKA > 3° from neutral) and the Knee Society Score and WOMAC scores at 6 months postoperatively. We combined direct and indirect comparisons using a Bayesian network meta-analysis framework to assess and compare the effect of different cutting guides on outcomes. Bayesian estimates are based on the posterior distribution of an endpoint and are called credible intervals. Usually the 95% credible interval, corresponding to a posterior probability of 0.95 that the endpoint lies in the interval, is computed. Unlike the frequentist approach, the Bayesian approach does not allow the calculation of the p value.
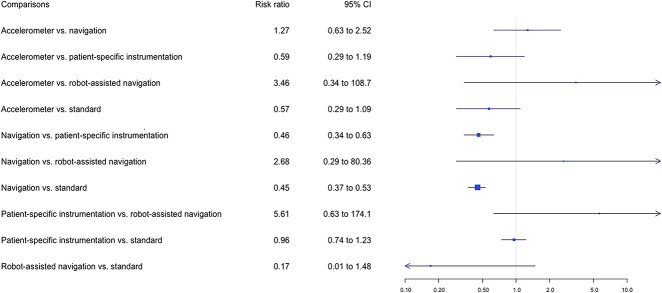
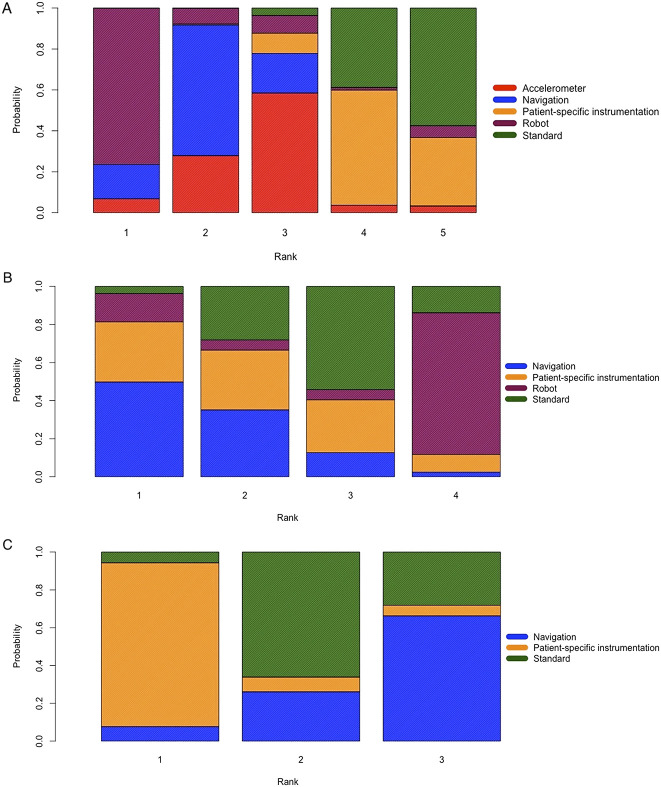
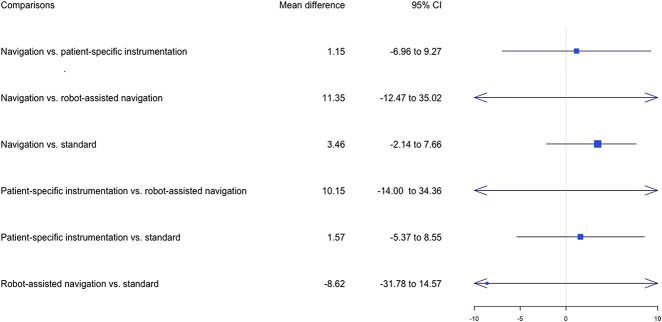
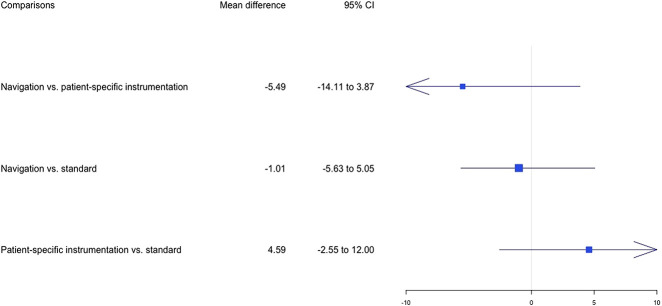
Results: The proportion of HKA outliers was lower with navigation than with patient-specific instrumentation (risk ratio 0.46 [95% credible interval (CI) 0.34 to 0.63]) and standard cutting guides (risk ratio 0.45 [95% CI 0.37 to 0.53]); however, this corresponded to an actual difference of only 12% of patients for navigation versus 21% of patients for patient-specific instrumentation, and 12% of patients for navigation versus 25% for standard cutting guides. We found no differences for other comparisons between different cutting guides, including robotics and the accelerometer. We found no differences in the Knee Society Score or WOMAC score between the different cutting guides at 6 months. Regarding secondary outcomes, navigation reduced the risk of frontal and sagittal malalignments for femoral and tibial components compared with the standard cutting guides, but none of the other cutting guides showed superiority for the other secondary outcomes.
Conclusions: Navigation resulted in approximately 10% fewer patients having HKA outliers of more than 3°, without any corresponding improvement in validated outcomes scores. It is unknown whether this incremental reduction in the proportion of patients who have alignment outside a window that itself has been called into question will justify the increased costs and surgical time associated with the approach. We believe that until or unless these new approaches either (1) convincingly demonstrate superior survivorship, or (2) convincingly demonstrate superior outcomes, surgeons and hospitals should not use these approaches since they add cost, have a learning curve (during which some patients may be harmed), and have the risks associated with uncertainty of novel surgical approaches.
Level of evidence: Level I, therapeutic study.
Conflict of interest statement
Each author certifies that neither he or she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures

Comment in
-
CORR Insights®: Are There Differences in Accuracy or Outcomes Scores Among Navigated, Robotic, Patient-specific Instruments or Standard Cutting Guides in TKA? A Network Meta-analysis.Clin Orthop Relat Res. 2020 Sep;478(9):2117-2119. doi: 10.1097/CORR.0000000000001399. Clin Orthop Relat Res. 2020. PMID: 32639308 Free PMC article. No abstract available.
References
-
- Banerjee S, Cherian JJ, Elmallah RK, Jauregui JJ, Pierce TP, Mont MA. Robotic-assisted knee arthroplasty. Expert Rev Med Devices. 2015;12:727–735. - PubMed
-
- Bauwens K Matthes G Wich M Gebhard F,Hanson B Ekkernkamp A,Stengel D, Navigated total knee replacement. A meta-analysis. J Bone Joint Surg Am. 2007;89:261-269. - PubMed
-
- Berger RA, Crossett LS, Jacobs JJ, Rubash HE. Malrotation causing patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res. 1998; 356:144–153. - PubMed
-
- Brooks SP, Gelman A. General Methods for Monitoring Convergence of Iterative Simulations. J Comput Graph Stat. 1998;7:434-355.
-
- Clark GW, Wood DJ. Robotics in arthroplasty: Where are we today? Bone & Joint 360 2015;4:2-7.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
