

Multimorbidity patterns, polypharmacy and their association with liver and kidney abnormalities in people over 65 years of age: a longitudinal study
- PMID: 32532213
- PMCID: PMC7291454
- DOI: 10.1186/s12877-020-01580-1
Multimorbidity patterns, polypharmacy and their association with liver and kidney abnormalities in people over 65 years of age: a longitudinal study
Erratum in
-
Correction to: Multimorbidity patterns, polypharmacy and their association with liver and kidney abnormalities in people over 65 years of age: a longitudinal study.BMC Geriatr. 2022 May 6;22(1):399. doi: 10.1186/s12877-021-02567-2. BMC Geriatr. 2022. PMID: 35524180 Free PMC article. No abstract available.
Abstract
Background: The implementation of individual clinical practice guidelines in patients with multimorbidity often results in polypharmacy. Our aim was to analyse medication use according to longitudinal multimorbidity patterns (MP) and determine during a 5-year period (2012-16) which MP are associated with abnormal liver and kidney function in primary care patients over 65 years of age living in Catalonia.
Methods: Design: Longitudinal study (years 2012 to 2016) based on the electronic health records contained in Information System for Research in Primary Care database of the Catalan Institute of Health (SIDIAP).
Variables: age, sex, MP, medication and polypharmacy (drug exposure obtained from the Pharmacy Invoice Registry). Medicines were classified in accordance with the Anatomical Therapeutic Chemical Classification System (ATC). Glomerular filtration rate was used to determine abnormal kidney function, and serum levels of alkaline phosphatase, alanine transaminase and gamma-glutamyl transpeptidase were used to diagnose abnormal liver function.
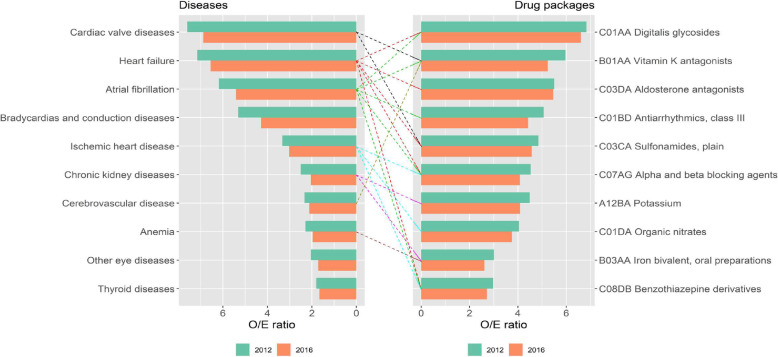
Statistics: For medication use in MP, we calculated annual mean packages of each drug in each MP, and observed/expected ratios were obtained by dividing mean packages in the cluster by mean packages of the same drug in the overall population. Logistic regression models were fitted to estimate the association between MP at baseline and abnormal kidney and liver function tests during follow up.
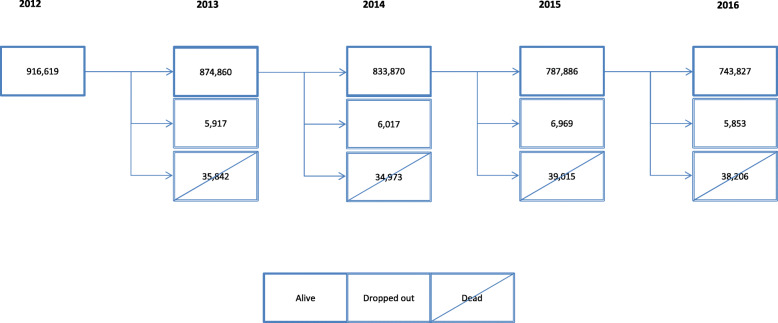
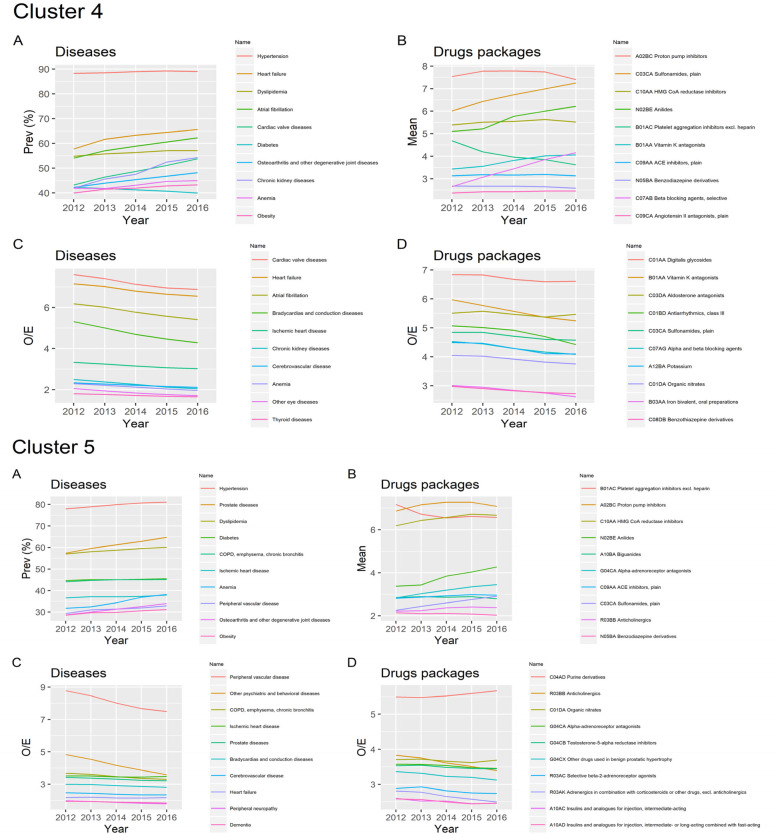
Results: Nine hundred sixteen thousand six hundred nineteen patients were included, and 743,827 completed the follow up. We identified one polypharmacy profile per MP, and concluded that the most prescribed drugs in each pattern corresponded to the diseases overrepresented in that specific MP. The median of drugs ranged from 3 (Cluster 1 - Non-Specific) to 8 (Cluster 10 - Multisystem Pattern). Abnormal kidney function was most commonly observed in the Cluster 4 - Cardio-Circulatory and Renal (Odds Ratio [OR] 2.19; Confidence interval [CI] 95% 2.15-2.23) and Cluster 3 - Minority Metabolic Autoimmune-Inflammatory (OR 2.16; CI 95% 2.12-2.20) MP. A higher risk of abnormal liver function was observed in the Cluster 8 - Digestive (OR 3.39; CI 95% 3.30-3.49), and Cluster 4 - Cardio-Circulatory and Renal (OR 1.96; CI 95% 1.91-2.02) MP.
Conclusions: A higher risk of abnormal kidney and liver function was observed in specific MP. The long-term characterisation of MP and polypharmacy illustrates the burden of chronic multimorbidity and polypharmacy in the elderly population.
Keywords: Ageing; Epidemiology; Longitudinal study; Multimorbidity; Polypharmacy; Primary health care.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Marengoni A, Angleman S, Melis R, Mangialasche F, Karp A, Garmen A, et al. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev. 2011;10(4):430–439. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
