

The impact of COVID-19 and strategies for mitigation and suppression in low- and middle-income countries
- PMID: 32532802
- PMCID: PMC7292504
- DOI: 10.1126/science.abc0035
The impact of COVID-19 and strategies for mitigation and suppression in low- and middle-income countries
Abstract
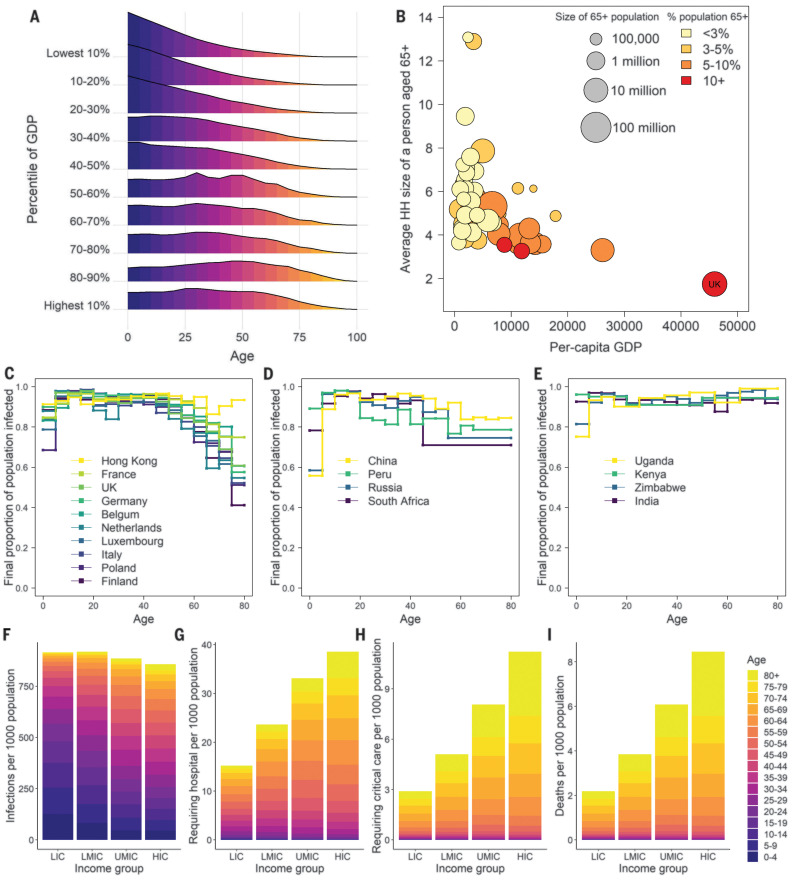
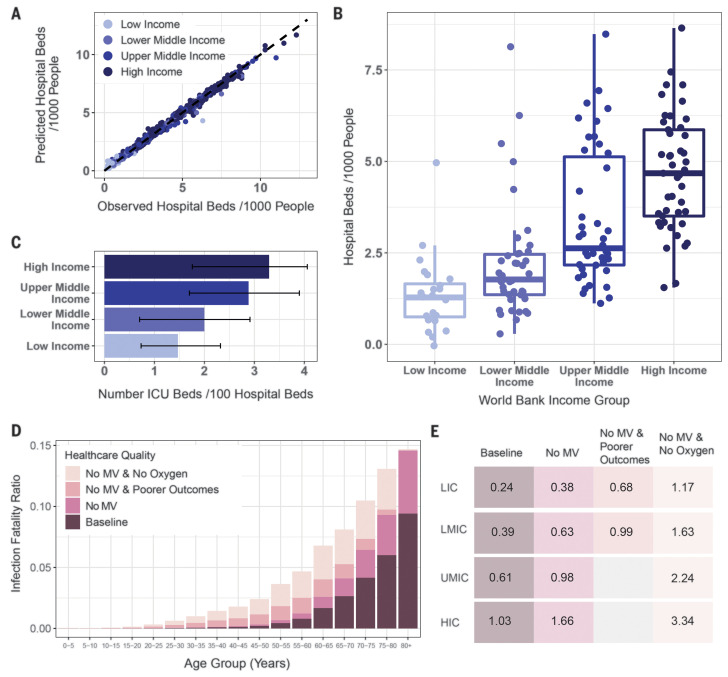
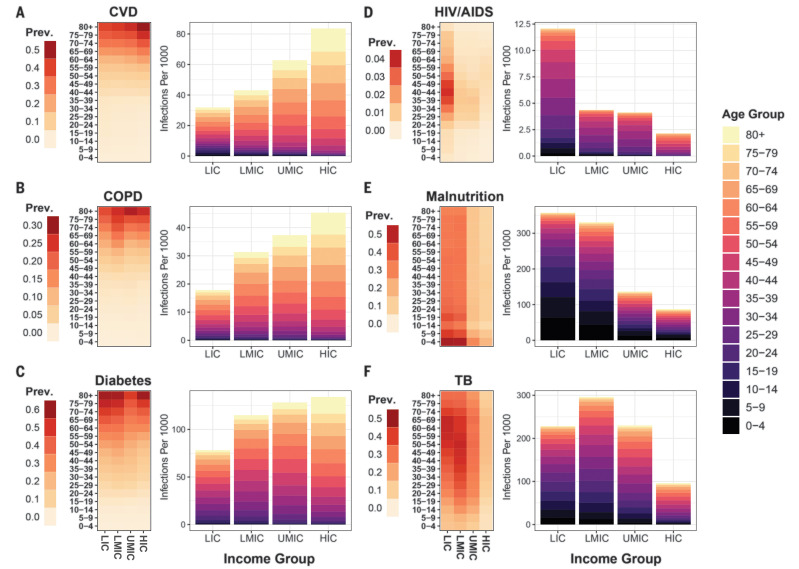
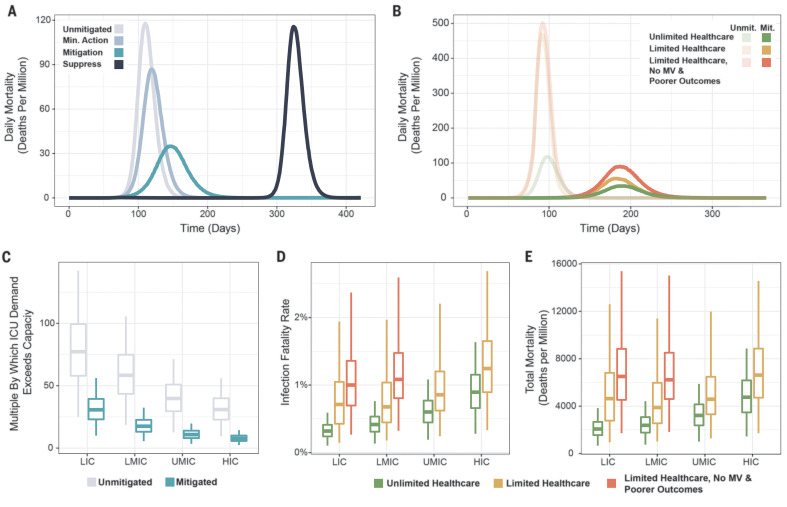
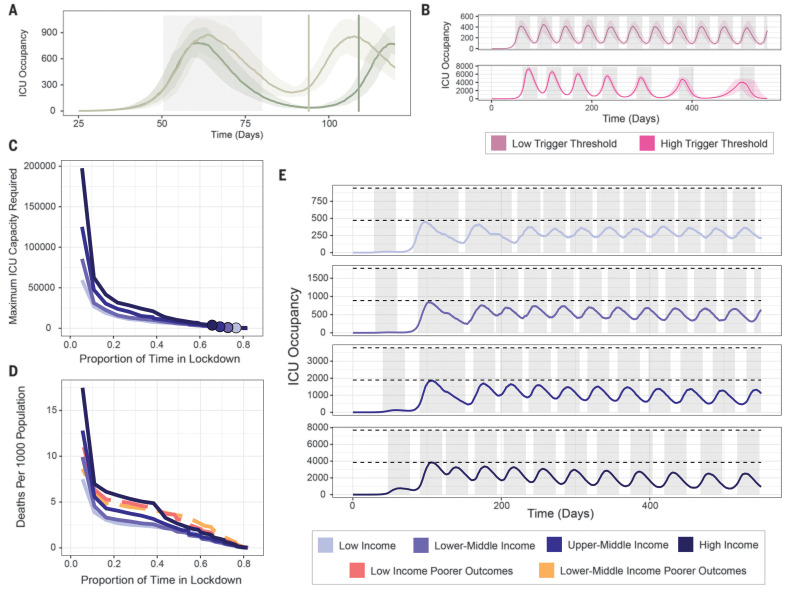
The ongoing coronavirus disease 2019 (COVID-19) pandemic poses a severe threat to public health worldwide. We combine data on demography, contact patterns, disease severity, and health care capacity and quality to understand its impact and inform strategies for its control. Younger populations in lower-income countries may reduce overall risk, but limited health system capacity coupled with closer intergenerational contact largely negates this benefit. Mitigation strategies that slow but do not interrupt transmission will still lead to COVID-19 epidemics rapidly overwhelming health systems, with substantial excess deaths in lower-income countries resulting from the poorer health care available. Of countries that have undertaken suppression to date, lower-income countries have acted earlier. However, this will need to be maintained or triggered more frequently in these settings to keep below available health capacity, with associated detrimental consequences for the wider health, well-being, and economies of these countries.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures
Comment in
-
Mathematical models to guide pandemic response.Science. 2020 Jul 24;369(6502):368-369. doi: 10.1126/science.abd1668. Science. 2020. PMID: 32703861 No abstract available.
References
-
- WHO, “Coronavirus disease (COVID-19) Situation Report-127” (2020); www.who.int/docs/default-source/coronaviruse/situation-reports/20200526-....
-
- Verity R., Okell L. C., Dorigatti I., Winskill P., Whittaker C., Imai N., Cuomo-Dannenburg G., Thompson H., Walker P. G. T., Fu H., Dighe A., Griffin J. T., Baguelin M., Bhatia S., Boonyasiri A., Cori A., Cucunubá Z., FitzJohn R., Gaythorpe K., Green W., Hamlet A., Hinsley W., Laydon D., Nedjati-Gilani G., Riley S., van Elsland S., Volz E., Wang H., Wang Y., Xi X., Donnelly C. A., Ghani A. C., Ferguson N. M., Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 20, 669–677 (2020). 10.1016/S1473-3099(20)30243-7 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
