

Aneurysm treatment with WEB in the cumulative population of two prospective, multicenter series: 3-year follow-up
- PMID: 32532858
- PMCID: PMC7982938
- DOI: 10.1136/neurintsurg-2020-016151
Aneurysm treatment with WEB in the cumulative population of two prospective, multicenter series: 3-year follow-up
Abstract
Background: WEB treatment is an endovascular approach for wide-neck bifurcation aneurysms that has demonstrated high safety and good efficacy in mid-term follow-up. While evaluating safety in the long term is important to determine if delayed adverse events occur affecting late morbidity and mortality, the most important point to evaluate is the long-term stability of aneurysm occlusion. The current analysis reports the 3-year clinical and anatomical results of WEB treatment in the combined population of two European trials (WEBCAST (WEB Clinical Assessment of Intrasaccular Aneurysm Therapy) and WEBCAST-2).
Methods: Aneurysm occlusion was evaluated using a 3-grade scale: complete occlusion, neck remnant, and aneurysm remnant.
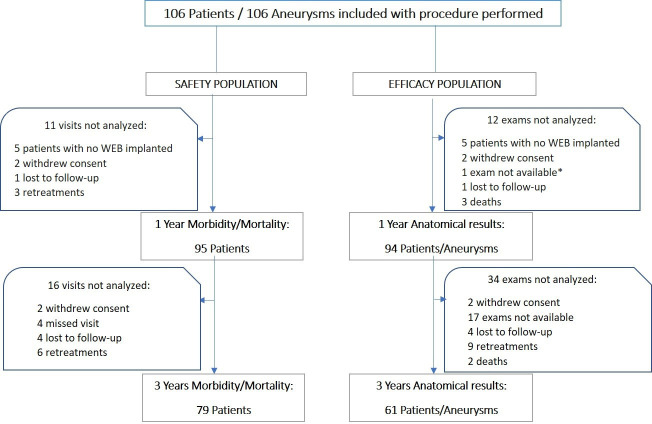
Results: The safety population comprised 79 patients. The efficacy population comprised 61 aneurysms. Aneurysm locations were middle cerebral artery in 32/61 aneurysms (52.5%), anterior communicating artery in 13/61 (21.3%), basilar artery in 9/61 (14.8%), and internal carotid artery terminus in 7/61 (11.5%). No adverse events related to the device or procedure occurred between 2 and 3 years. At 3 years, complete occlusion was observed in 31/61 (50.8%) aneurysms, neck remnant in 20/61 (32.8%), and aneurysm remnant in 10/61 (16.4%). Between 1 year and 3 years, aneurysm occlusion was improved or stable in 53/61 (86.9%) aneurysms and worsened in 8/61 (13.1%). Worsening was mostly from complete occlusion to neck remnant in 6/61 (9.8%) aneurysms. The retreatment rate at 3 years was 11.4%.
Conclusions: This analysis confirms the high safety profile of WEB. Moreover, evidence demonstrates the great stability of aneurysm occlusion with adequate occlusion (complete occlusion or neck remnant) in 83.6% of aneurysms.
Clinical trial registration: URL: http://www.clinicaltrials.gov. WEBCAST and WEBCAST-2: Unique identifier: NCT01778322.
Keywords: aneurysm.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: LP consults for Balt, MicroVention, Neuravi, and Penumbra. ISI consults for Codman, Medtronic, Sequent, and Stryker. XB consults for MicroVention and Stryker. LS consults for Stryker, MicroVention, Medtronic, and Balt. JF has received fees as consultant or lecturer from Acandis, Bayer, Boehringer-Ingelheim, Codman, Covidien, MicroVention, Penumbra, Philips, Sequent, Siemens, and Stryker; his institution received funding from MicroVention, Medtronic, BMBF, BMWi, DFG, and the EU. VC consults for MicroVention and Balt, and receives educational grants from Medtronic and Stryker. JK consults for MicroVention/Sequent. WW consults for MicroVention, Phenox, and Medtronic. TL consults for Medtronic, Mentice, Microvention, and Route 92. JM consults for Medtronic, MicroVention, Stryker, and Balt. AM consults for MicroVention/Sequent and Cerus Endovascular. JB consults for, and is shareholder of, Oxford Endovascular Ltd; his institution received funding from MicroVention.
Figures
References
-
- Pierot L, Barbe C, Nguyen HA, et al. . Intraoperative complications of endovascular treatment of intracranial aneurysms with coiling or balloon-assisted coiling in a prospective multicenter cohort of 1088 participants: analysis of recanalization after endovascular treatment of intracranial aneurysm (ARETA) study. Radiology 2020;295:381–9. 10.1148/radiol.2020191842 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical