

The competitive athlete with type 1 diabetes
- PMID: 32533229
- PMCID: PMC7351823
- DOI: 10.1007/s00125-020-05183-8
The competitive athlete with type 1 diabetes
Abstract
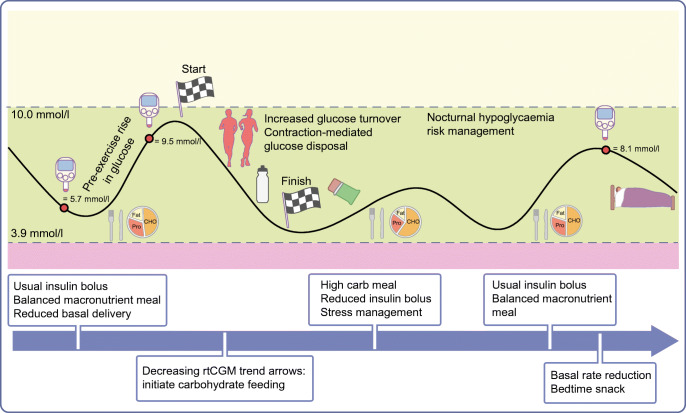
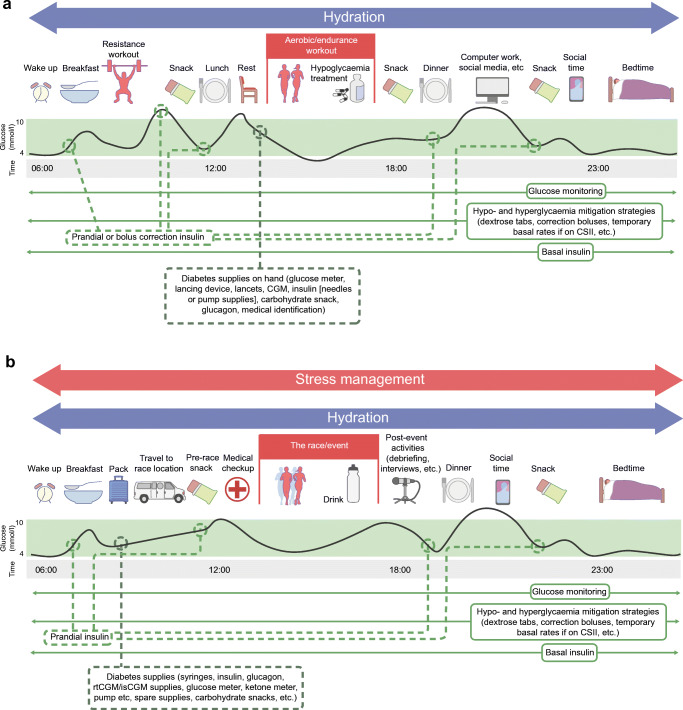
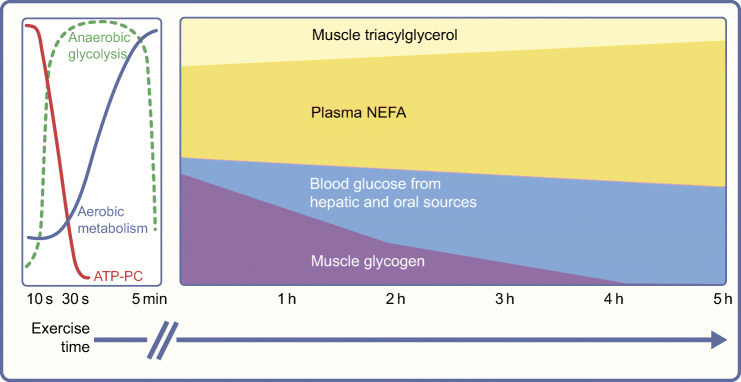
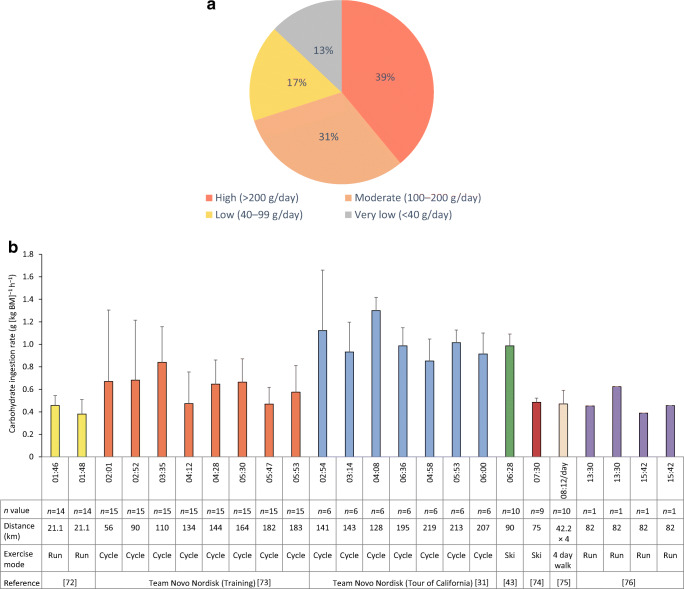
Regular exercise is important for health, fitness and longevity in people living with type 1 diabetes, and many individuals seek to train and compete while living with the condition. Muscle, liver and glycogen metabolism can be normal in athletes with diabetes with good overall glucose management, and exercise performance can be facilitated by modifications to insulin dose and nutrition. However, maintaining normal glucose levels during training, travel and competition can be a major challenge for athletes living with type 1 diabetes. Some athletes have low-to-moderate levels of carbohydrate intake during training and rest days but tend to benefit, from both a glucose and performance perspective, from high rates of carbohydrate feeding during long-distance events. This review highlights the unique metabolic responses to various types of exercise in athletes living with type 1 diabetes. Graphical abstract.
Keywords: Athlete; Carbohydrate; Competition; Continuous glucose monitoring; Exercise; Glucose; Insulin; Nutrition; Review; Sport; Type 1 diabetes.
Figures

References
-
- Stadler M, Peric S, Strohner-Kaestenbauer H, et al. Mortality and incidence of renal replacement therapy in people with type 1 diabetes mellitus–a three decade long prospective observational study in the Lainz T1DM cohort. J Clin Endocrinol Metab. 2014;99(12):4523–4530. doi: 10.1210/jc.2014-2701. - DOI - PubMed
