

Treatment outcomes after splenectomy with gastric devascularization or balloon-occluded retrograde transvenous obliteration for gastric varices: a propensity score-weighted analysis from a single institution
- PMID: 32533300
- PMCID: PMC7289714
- DOI: 10.1007/s00535-020-01693-9
Treatment outcomes after splenectomy with gastric devascularization or balloon-occluded retrograde transvenous obliteration for gastric varices: a propensity score-weighted analysis from a single institution
Abstract
Background: Although balloon-occluded retrograde transvenous obliteration (BRTO) is often selected to treat gastric varices caused by portal hypertension, data comparing BRTO and splenectomy with gastric devascularization (Sp + Dev) are limited.
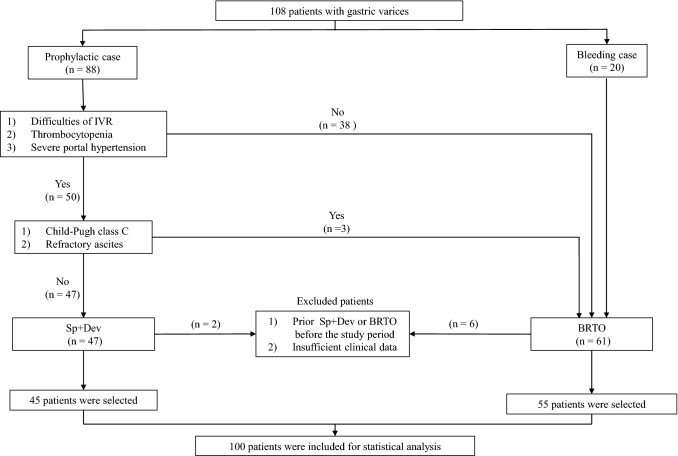
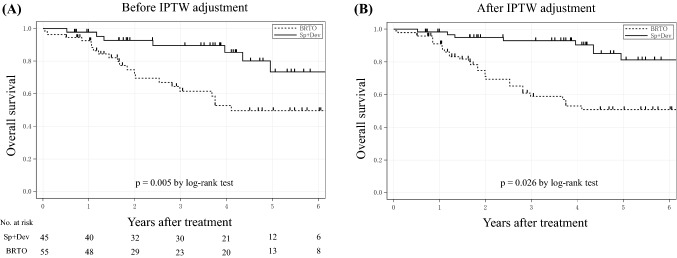
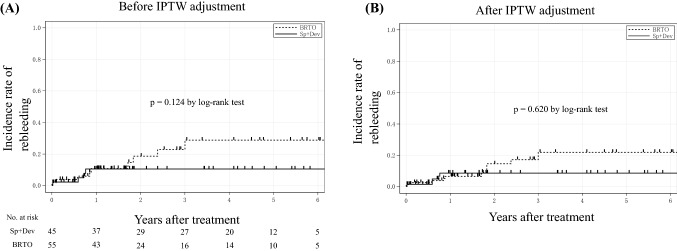
Methods: From January 2009 to February 2018, 100 patients with gastric varices caused by portal hypertension who underwent Sp + Dev (n = 45) or BRTO (n = 55) were included. Overall survival (OS) and the rebleeding rate were calculated using the inverse probability of a treatment weighting-adjusted log-rank test. Independent risk factors were identified by Cox regression analysis. Changes in liver function and adverse events after the procedures were analyzed.
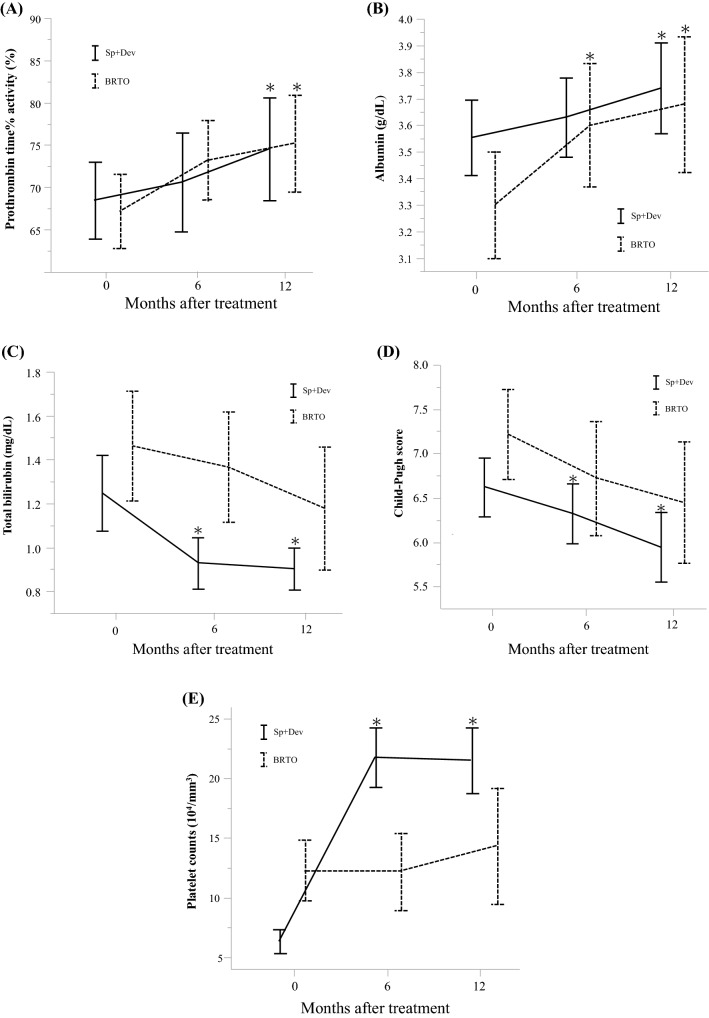
Results: Patients in the Sp + Dev group tended to have lower platelet counts than those in the BRTO group, but liver function did not differ between these groups. The 5-year OS rates for the Sp + Dev and BRTO groups were 73.4 and 50.0% (p = 0.005), respectively. There were no significant differences in rebleeding rates between the two groups. Multivariate analysis showed that serum albumin level ≤3.6 g/dL, prothrombin time% activity (PT%) ≤80%, and serum creatinine level ≥0.84 mg/dL were poor prognostic factors. Although the Sp + Dev group had more short-term complications after procedures, Sp + Dev tended to be more effective in improving liver function than BRTO.
Conclusions: Sp + Dev showed better OS and improvement of liver function compared with BRTO for the treatment of gastric varices caused by portal hypertension.
Keywords: Balloon-occluded transvenous obliteration; Gastric devascularization; Gastric varices; Portal hypertension; Splenectomy.
Conflict of interest statement
The authors declare that they have no conflicts of interest concerning this article.
Figures
References
-
- Hassab MA. Gastroesophageal decongestion and splenectomy in the treatment of esophageal varices in bilharzial cirrhosis: further studies with a report on 355 operations. Surgery. 1967;61:169–176. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
