

Systematic review of the emerging literature on the effectiveness of naloxone access laws in the United States
- PMID: 32533570
- PMCID: PMC8051142
- DOI: 10.1111/add.15163
Systematic review of the emerging literature on the effectiveness of naloxone access laws in the United States
Abstract
Background and aims: Naloxone access laws (NALs) have been suggested to be an important strategy to reduce opioid-related harm. We describe the evolution of NALs across states and over time and review existing evidence of their overall association with naloxone distribution and opioid overdose as well as the potential effects of specific NAL components.
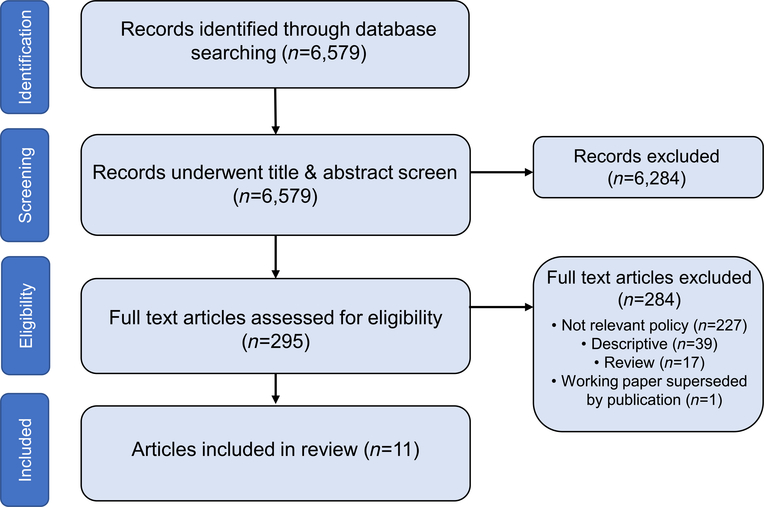
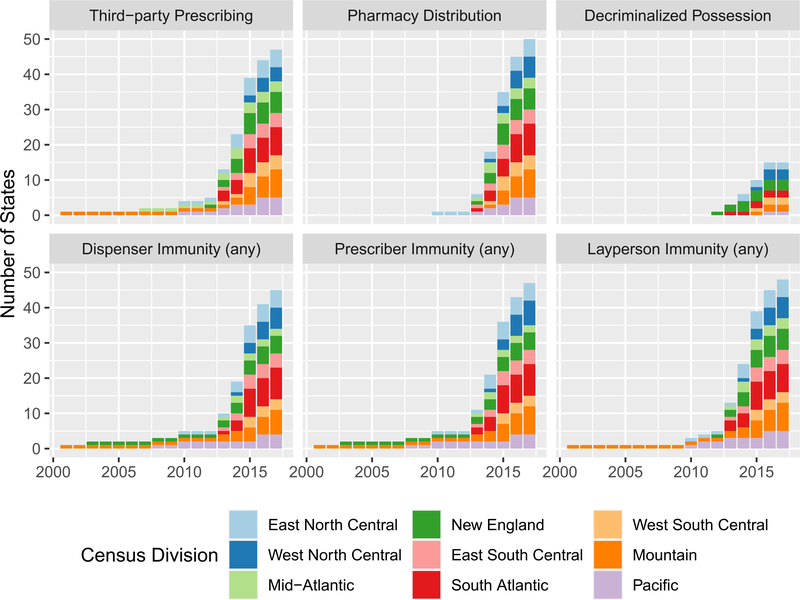
Methods: Descriptive analysis of temporal variation in US regional adoption of NAL components, accompanied by a systematic search of 13 databases for studies (published between 2005 and 20 December 2019) assessing the effects of NALs on naloxone distribution or opioid-related health outcomes. Eleven studies, all published since 2018, met inclusion criteria. Study time-frames spanned 1999-2017. Opioid-related overdose mortality, emergency department episodes and naloxone distribution were correlated with the presence of a NAL and, where data were available, NAL components.
Results: Existing evidence suggests mixed, but generally beneficial, effects for NALs. Nearly all studies show that NALs, particularly those that permit naloxone distribution without patient-specific prescriptions, are associated with increased naloxone access [incidence rate ratios (IRR) range from 1.40, 95% confidence interval (CI) = 1.15-1.66 to 7.75, 95% CI = 1.22-49.35] and increased opioid-related emergency department visits (IRR range from 1.14, 95% CI = 1.07-1.20 to 1.15, 95% CI = 1.02-1.29). Most studies show NALs are associated with reduced overdose mortality, although findings vary depending on the specific NAL components and time-period analyzed (IRR range from 0.66, 95% CI = 0.42-0.90 to 1.27, 95% CI = 1.27-1.27). Few studies account for the variation in opioid environments (i.e. illicit versus prescription) or other policy dimensions that may be correlated with outcomes.
Conclusions: The existing literature on naloxone access laws in the United States supports beneficial effects for increased naloxone distribution, but provides inconclusive evidence for reduced fatal opioid overdose. Mixed findings may reflect variation in the laws' design and implementation, confounding effects of concurrent policy adoption, or differential effectiveness in light of changing opioid environments.
Keywords: Harm reduction; mortality; naloxone; opioids; overdose; pharmacy.
© 2020 Society for the Study of Addiction.
Figures
References
-
- McDonald R, Campbell ND, Strang J Twenty years of take-home naloxone for the prevention of overdose deaths from heroin and other opioids—conception and maturation. Drug Alcohol Depend 2017; 178: 176–87. - PubMed
-
- Davis CS, Carr D Legal changes to increase access to naloxone for opioid overdose reversal in the United States. Drug Alcohol Depend 2015; 157: 112–20. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
