

Recognizing genetic disease: A key aspect of pediatric pulmonary care
- PMID: 32533909
- PMCID: PMC7384240
- DOI: 10.1002/ppul.24706
Recognizing genetic disease: A key aspect of pediatric pulmonary care
Abstract
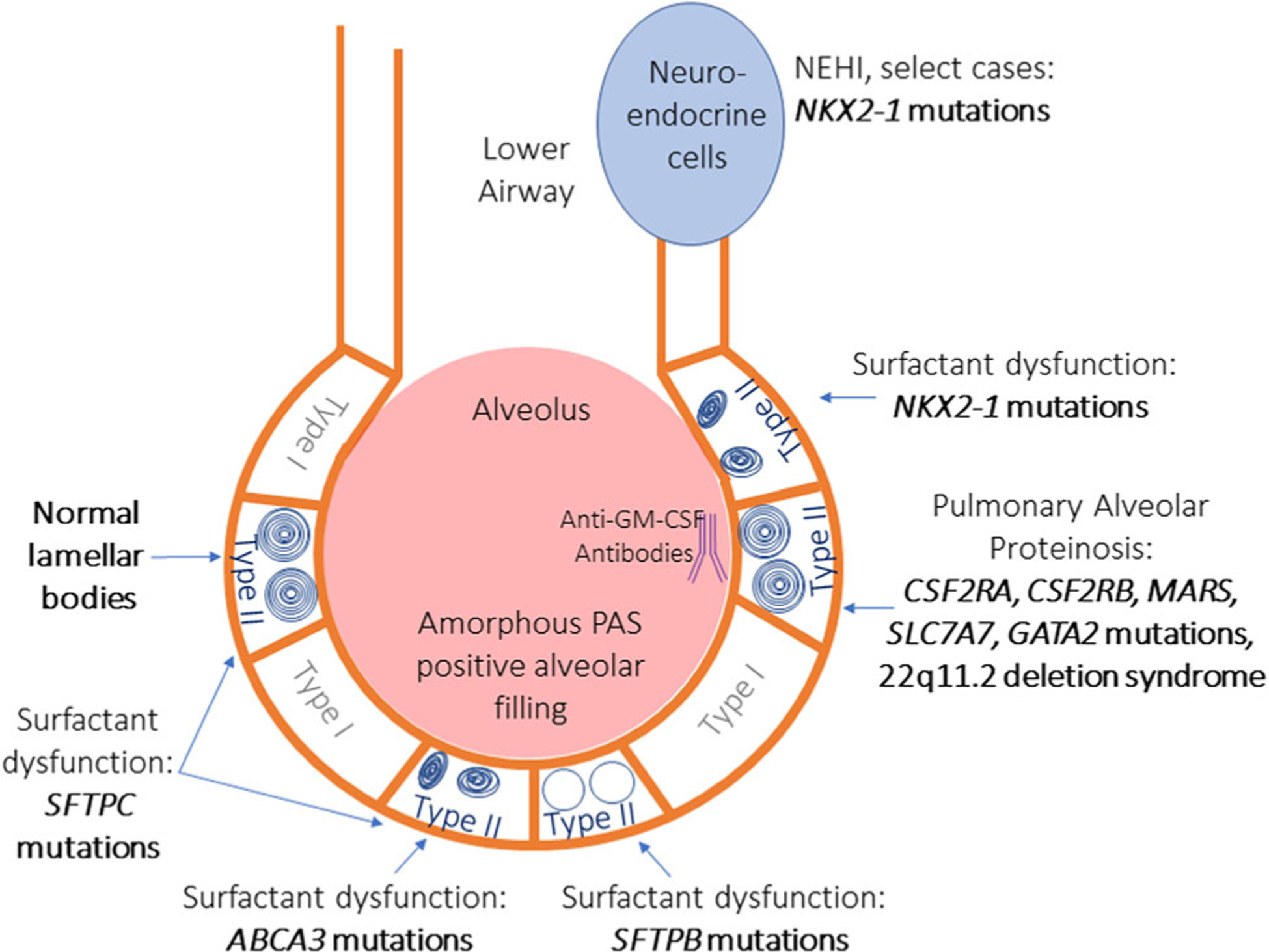
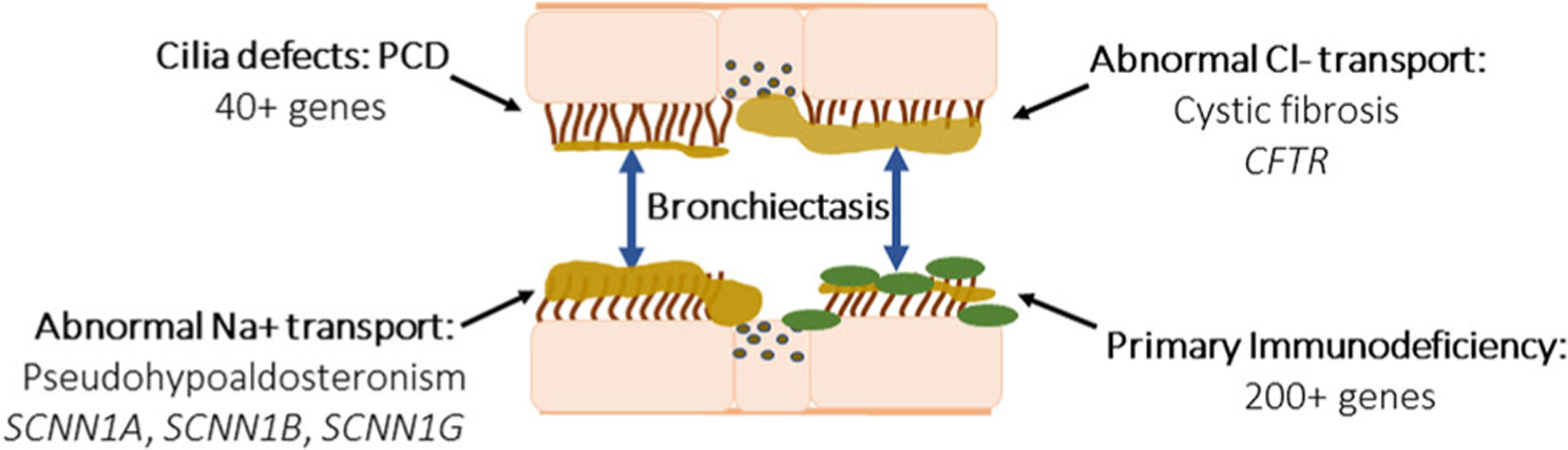
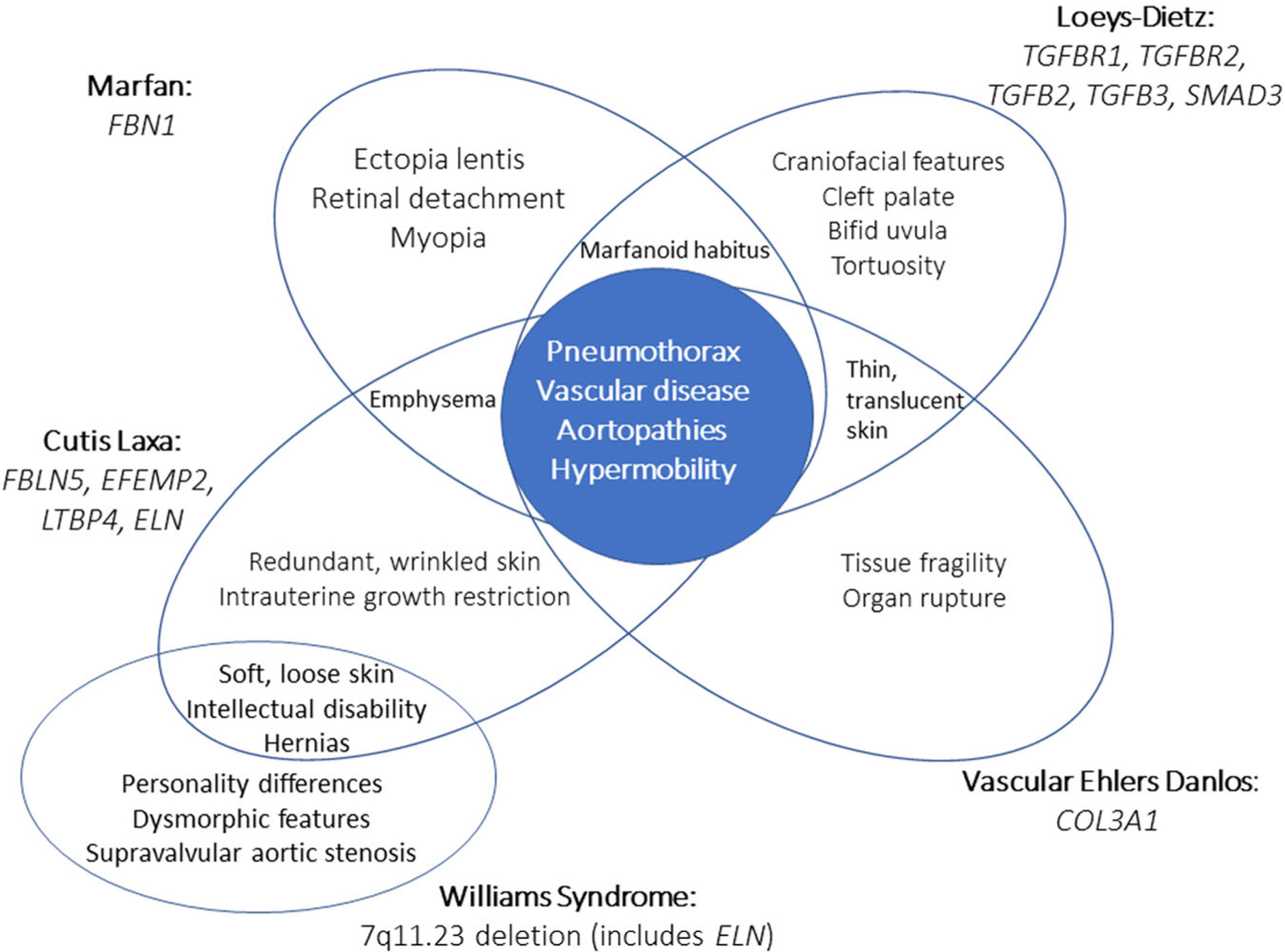
Advancement in technology has improved recognition of genetic etiologies of disease, which has impacted diagnosis and management of rare disease patients in the pediatric pulmonary clinic. This review provides an overview of genetic conditions that are likely to present with pulmonary features and require extensive care by the pediatric pulmonologist. Increased familiarity with these conditions allows for improved care of these patients by reducing time to diagnosis, tailoring management, and prompting further investigation into these disorders.
Keywords: bronchiectasis and primary ciliary dyskinesia; cystic fibrosis (CF); genetics/Genome-Wide Association Studies (GWAS); immunology and immunodeficiency; surfactant biology and pathophysiology.
© 2020 Wiley Periodicals, Inc.
Figures
References
-
- Griese M Pulmonary surfactant in health and human lung diseases: state of the art. Eur Respir J. 1999;13(6):1455–1476. - PubMed
-
- Liszewski MC, Stanescu AL, Phillips GS, Lee EY. Respiratory distress in neonates: underlying causes and current imaging assessment. Radiol Clin North Am. 2017;55(4):629–644. - PubMed
-
- Nattes E, Lejeune S, Carsin A, et al. Heterogeneity of lung disease associated with NK2 homeobox 1 mutations. Respir Med. 2017;129: 16–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
