

Acute Kidney Function Declines in the Context of Decongestion in Acute Decompensated Heart Failure
- PMID: 32535124
- PMCID: PMC9027677
- DOI: 10.1016/j.jchf.2020.03.009
Acute Kidney Function Declines in the Context of Decongestion in Acute Decompensated Heart Failure
Abstract
Objectives: This study aimed to examine whether incorporation of a comprehensive set of measures of decongestion modifies the association of acute declines in kidney function with outcomes.
Background: In-hospital acute declines in kidney function occur in approximately 20% to 30% of patients admitted with acute decompensated heart failure (ADHF) and may be associated with adverse outcomes.
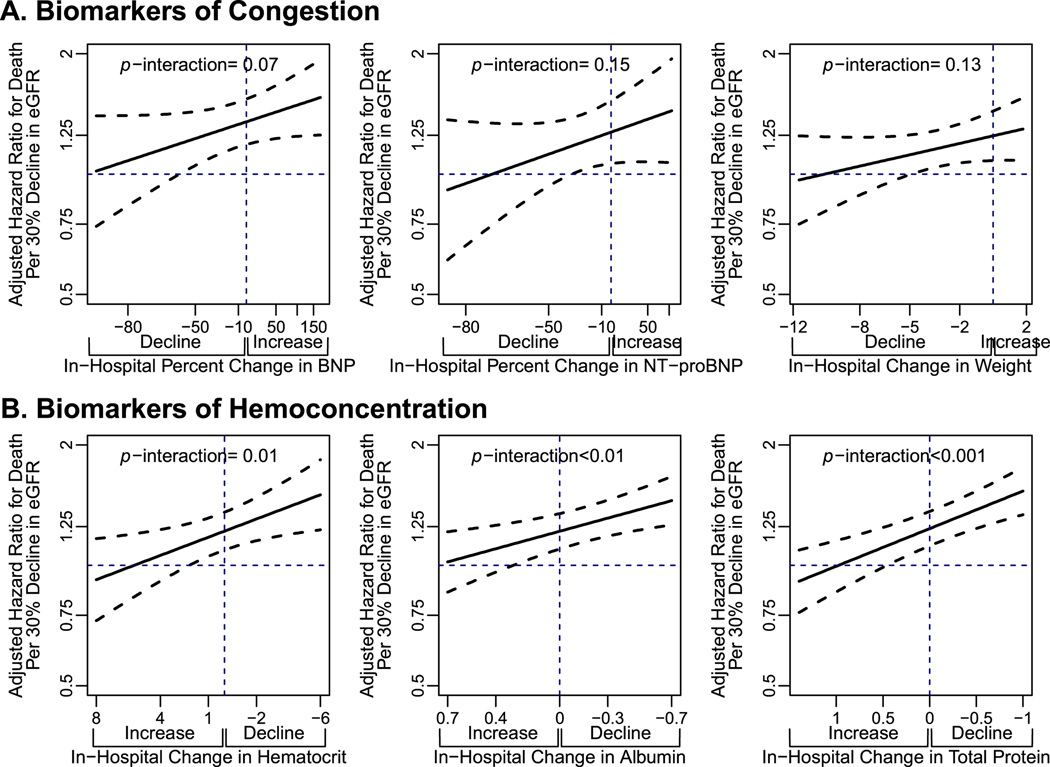
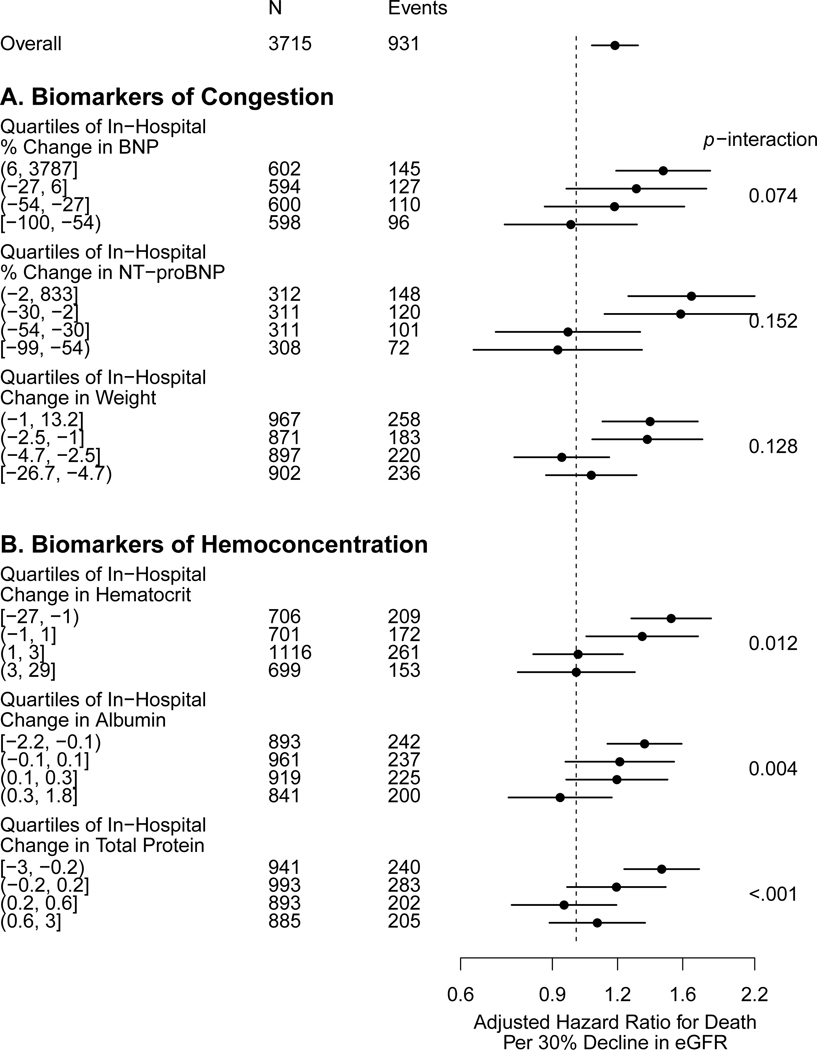
Methods: Using data from EVEREST (Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan), we used multivariable Cox regression models to evaluate the association between in-hospital changes in estimated glomerular filtration rate (eGFR) with death and a composite outcome of cardiovascular death and hospitalization for heart failure. We evaluated eGFR declines within the context of changes in markers of volume overload including b-type natriuretic peptide (BNP), N-terminal prohormone of B-type natriuretic peptide (NT-proBNP), and weight, as well as changes in measures of hemoconcentration including hematocrit, albumin, and total protein.
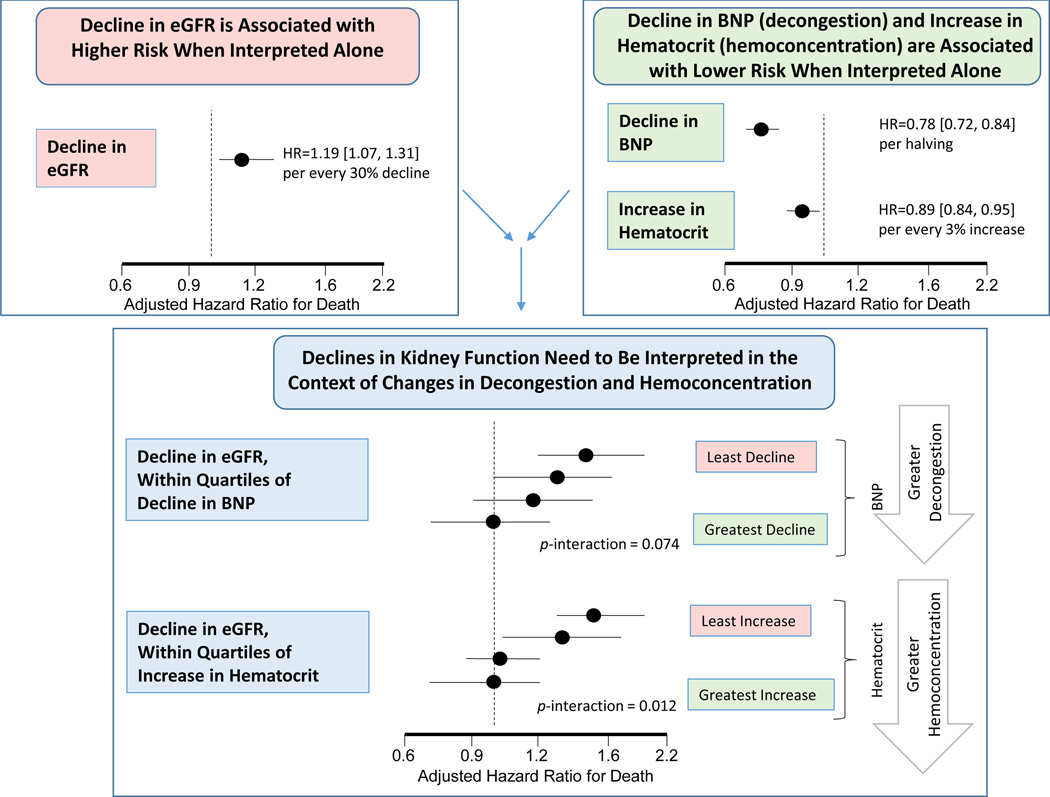
Results: Among 3,715 patients over a median follow-up of 9.9 months, every 30% decline in eGFR was associated with higher risk of both death (hazard ratio [HR]: 1.19; 95% confidence interval [CI]: 1.07 to 1.31) and the composite outcome (HR: 1.09; 95% CI: 1.01 to 1.18) in adjusted models. The acute decline in eGFR was no longer associated with higher risk of either outcome as long as there was evidence of decongestion, either by declines in BNP, NT-proBNP, or weight or by increases in hematocrit, albumin or total protein. Interaction testing between decline in eGFR and changes in hematocrit, albumin, and total protein was statistically significant (p interaction of <0.01 for death and p interaction of ≤0.01 for composite for all 3 biomarkers). Interaction between change in eGFR and changes in BNP (p interaction = 0.07 for death; p interaction = 0.08 for composite), NT-proBNP (p interaction = 0.15 for death; p interaction = 0.18 for composite) and weight (p interaction = 0.13 for death; p interaction = 0.19 for composite) did not meet statistical significance.
Conclusions: Overall, acute declines in eGFR are associated with adverse outcomes, with evidence of modification by changes in markers of decongestion, suggesting that they are no longer associated with adverse outcomes if these markers are concomitantly improving.
Keywords: cardiorenal; decongestion; hemoconcentration; worsening renal function.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Damman K, Navis G, Voors AA, et al. Worsening renal function and prognosis in heart failure: systematic review and meta-analysis. J. Card. Fail 2007;13:599–608. - PubMed
-
- Forman DE, Butler J, Wang Y, et al. Incidence, predictors at admission, and impact of worsening renal function among patients hospitalized with heart failure. J. Am. Coll. Cardiol 2004;43:61–67. - PubMed
-
- Damman K, van Deursen VM, Navis G, Voors AA, van Veldhuisen DJ, Hillege HL. Increased central venous pressure is associated with impaired renal function and mortality in a broad spectrum of patients with cardiovascular disease. J. Am. Coll. Cardiol 2009;53:582–588. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
