

Current practice in the management of acromioclavicular joint dislocations; a national survey in the Netherlands
- PMID: 32535639
- PMCID: PMC8476372
- DOI: 10.1007/s00068-020-01414-0
Current practice in the management of acromioclavicular joint dislocations; a national survey in the Netherlands
Abstract
Purpose: The aim of this study was to investigate current practice in the management of acromioclavicular joint dislocations in the Netherlands.
Methods: A 36-item literature-based and expert consensus survey was developed. If available, one orthopaedic and one trauma surgeon for every hospital (n = 82) in the Netherlands was asked to complete the online questionnaire. Only complete data sets were included in the analysis. Descriptive analysis was performed using SPSS.
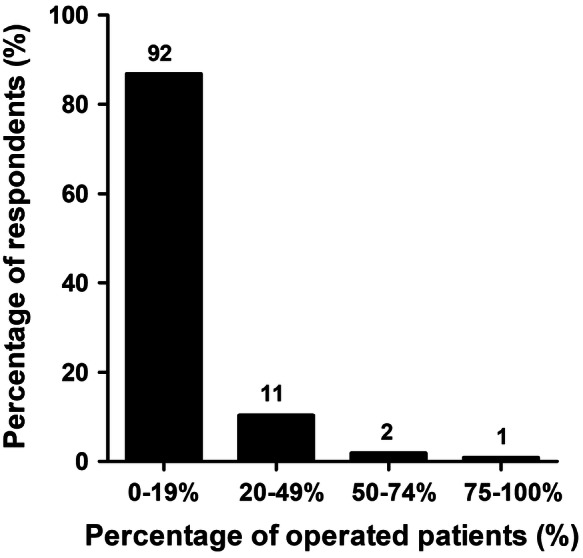
Results: Of 149 invited surgeons, 106 (71%) fully completed the survey. The diagnosis of ACJ injury was mainly based on physical examination (91%) and radiographs (95%). The vast majority of patients with ACJ injuries was treated non-operatively. The decision for operative treatment was mainly based on the surgeon's experience and available literature. Patient-related factors that contributed most to the decision to operate or not, were mainly functional needs and age. Cosmesis and gender contributed less to this decision. Rockwood II and III ACJ injuries were usually treated non-operatively, whereas Rockwood IV and V ACJ injuries were usually treated operatively. For primary and secondary operative treatment, a flexible implant was preferred over rigid fixation techniques. All respondents agreed that nonoperative treatment of Rockwood II ACJ injuries leads to satisfactory results and that secondary operative treatment is only rarely required. Also the majority of patients with Rockwood III ACJ injuries is treated non-operatively, although failure rates are considered higher.
Conclusion: This survey showed a significant individual variation on diagnosis and treatment strategies among surgeons in the Netherlands. The majority of the Dutch surgeons concern a flexible implant the best available technique for patients who require operative treatment.
Keywords: ACJ injury; Acromio-clavicular joint; Rockwood; Shoulder; Survey; Trauma.
© 2020. The Author(s).
Conflict of interest statement
PP. De Rooij, E.M.M. Van Lieshout, I.J. Schurink, and M.H.J. Verhofstad declare that they have no conflict of interest.
Figures








References
-
- Buckholz RW, Heckman JD. Rockwood and Green’s fracture in adults. 5. Philadelphia: Lippincott Williams & Wilkins; 2001. pp. 1210–1244.
-
- Allemann F, Halvachizadeh S, Waldburger M, Schaefer F, Pothmann C, Pape HC, et al. Different treatment strategies for acromioclavicular dislocation injuries: a nationwide survey on open/minimally invasive and arthroscopic concepts. Eur J Med Res. 2019;24(1):18. doi: 10.1186/s40001-019-0376-7. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
