

Comparison of the regenerative effects of bone marrow/adipose-derived stem cells in the Asherman model following local or systemic administration
- PMID: 32535814
- PMCID: PMC7468039
- DOI: 10.1007/s10815-020-01856-w
Comparison of the regenerative effects of bone marrow/adipose-derived stem cells in the Asherman model following local or systemic administration
Abstract
Purpose: Cell therapy is a promising strategy for the treatment of Asherman's syndrome (AS), but the origin of these cells and injection route influence the therapeutic effect and complications of cell therapy. Herein, we compared the effects of systemic or local intrauterine injection of bone marrow or adipose-derived mesenchymal stem cells (BMSCs/AMSCs) on the endometrium in a rat model of AS.
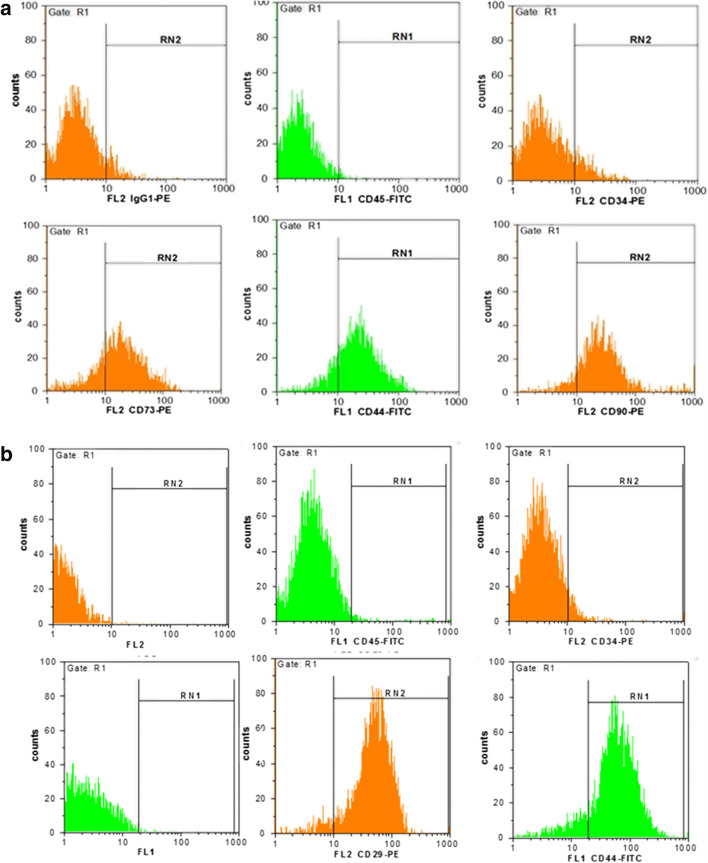
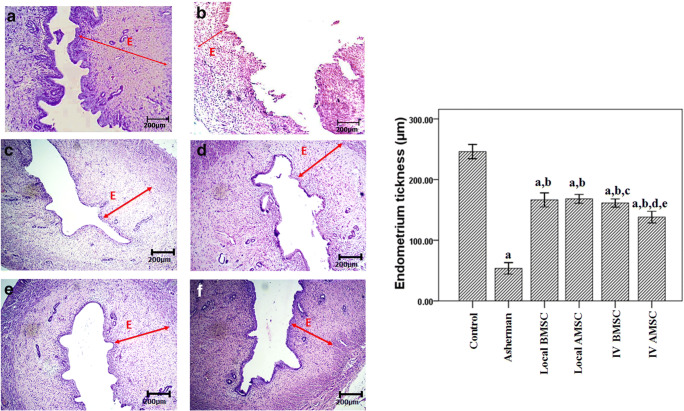
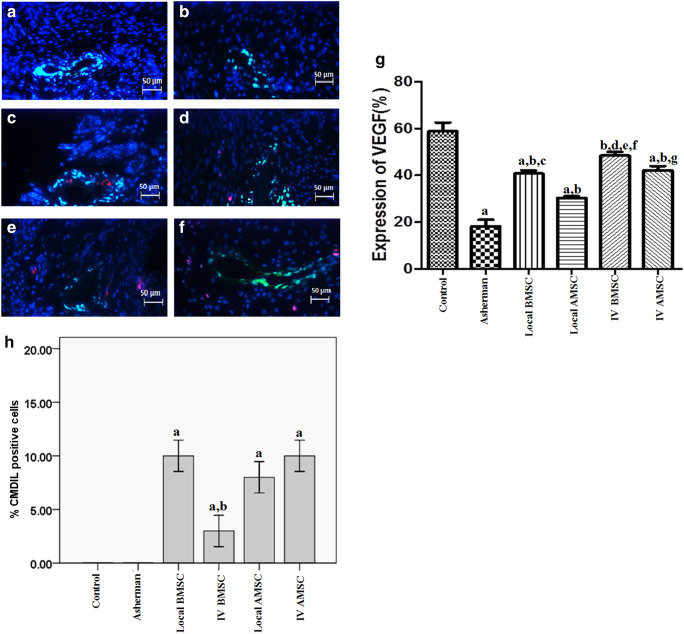
Methods: After induction of AS in adult Wistar rats, the CM-Dil-positive BMSCs or AMSCs were injected either locally or intravenously. After 3 weeks, endometrial thickness, collagen deposition, cell migration, and VEGF expression were evaluated using histochemistry/immunofluorescence studies.
Results: In all stem cell-treated groups, an ameliorative effect on the damaged endometrium was noted. Collagen deposition diminished in both groups (IV and local injection) compared to the AS model. In rats injected locally with MSC, fibrosis decreased compared to the other groups. Moreover, endometrial thickness increased in the groups that received local injection of BMSCs and AMSCs more than the IV-transplanted AMSCs group. Immunofluorescent staining demonstrated that although the systemic transplantation of BMSCs was more effective than the other groups on VEGF expression, it led to the lowest number of CM-Dil+ stem cells in the damaged endometrium.
Conclusion: Stem cell transplantation may reconstruct the damaged endometrium, but it is recommended to select the most effective stem cells and injection route. Because the removal of the fibrosis and the replacement of the epithelia cells is an effective therapeutic strategy for AS, in this study, we conclude that the local injection of AMSCs is more appropriate than BMSCs to treat AS.
Keywords: Adipose-derived mesenchymal stem cell; Asherman’s syndrome; Bone marrow-derived mesenchymal stem cell; Endometrium.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

References
-
- Westendorp IC, Ankum WM, Mol BW, Vonk J. Prevalence of Asherman’s syndrome after secondary removal of placental remnants or a repeat curettage for incomplete abortion. Human Reprod. 1998;13(12):3347–50. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
