

Risk of pneumococcal bacteremia in Kenyan children with glucose-6-phosphate dehydrogenase deficiency
- PMID: 32536341
- PMCID: PMC7294654
- DOI: 10.1186/s12916-020-01604-y
Risk of pneumococcal bacteremia in Kenyan children with glucose-6-phosphate dehydrogenase deficiency
Abstract
Background: Glucose-6-phosphate dehydrogenase (G6PD) deficiency is the most common enzyme deficiency state in humans. The clinical phenotype is variable and includes asymptomatic individuals, episodic hemolysis induced by oxidative stress, and chronic hemolysis. G6PD deficiency is common in malaria-endemic regions, an observation hypothesized to be due to balancing selection at the G6PD locus driven by malaria. G6PD deficiency increases risk of severe malarial anemia, a key determinant of invasive bacterial disease in malaria-endemic settings. The pneumococcus is a leading cause of invasive bacterial infection and death in African children. The effect of G6PD deficiency on risk of pneumococcal disease is undefined. We hypothesized that G6PD deficiency increases pneumococcal disease risk and that this effect is dependent upon malaria.
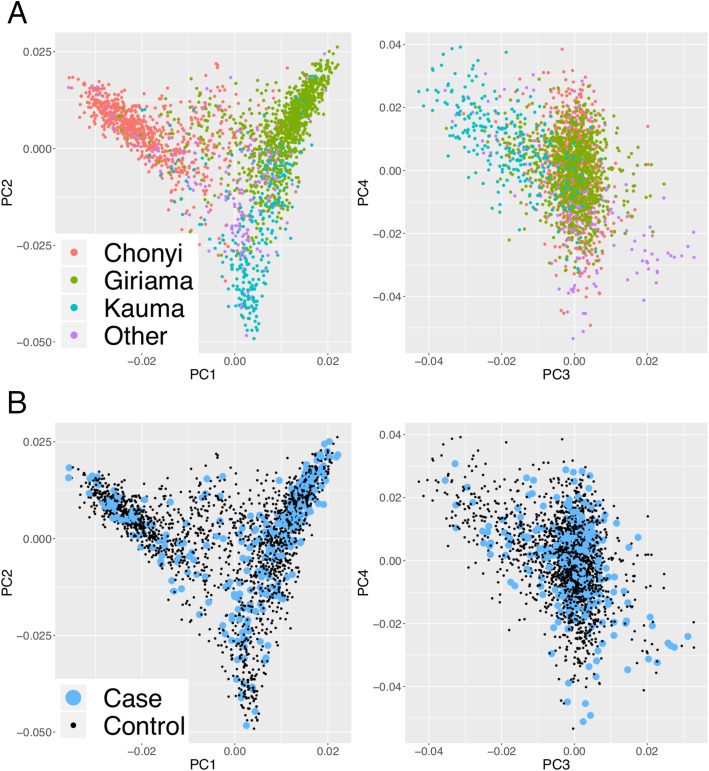
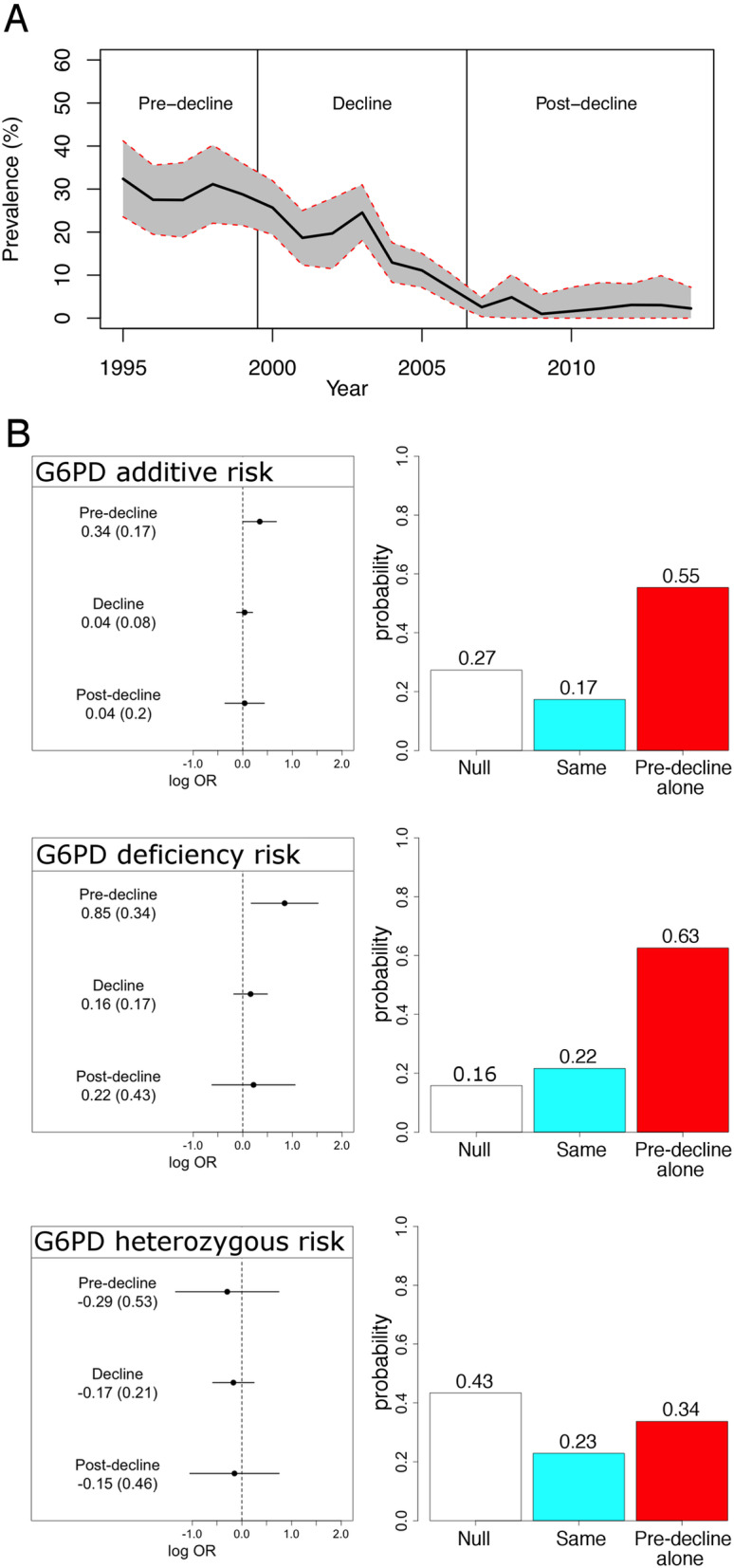
Methods: We performed a genetic case-control study of pneumococcal bacteremia in Kenyan children stratified across a period of falling malaria transmission between 1998 and 2010.
Results: Four hundred twenty-nine Kenyan children with pneumococcal bacteremia and 2677 control children were included in the study. Among control children, G6PD deficiency, secondary to the rs1050828 G>A mutation, was common, with 11.2% (n = 301 of 2677) being hemi- or homozygotes and 33.3% (n = 442 of 1329) of girls being heterozygotes. We found that G6PD deficiency increased the risk of pneumococcal bacteremia, but only during a period of high malaria transmission (P = 0.014; OR 2.33, 95% CI 1.19-4.57). We estimate that the population attributable fraction of G6PD deficiency on risk of pneumococcal bacteremia in areas under high malaria transmission is 0.129.
Conclusions: Our data demonstrate that G6PD deficiency increases risk of pneumococcal bacteremia in a manner dependent on malaria. At the population level, the impact of G6PD deficiency on invasive pneumococcal disease risk in malaria-endemic regions is substantial. Our study highlights the infection-associated morbidity and mortality conferred by G6PD deficiency in malaria-endemic settings and adds to our understanding of the potential indirect health benefits of improved malaria control.
Keywords: Africa; Bacteremia; Children; G6PD deficiency; Malaria; Pneumococcus.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
