

Indocyanine Green Angiography in Breast Reconstruction: Utility, Limitations, and Search for Standardization
- PMID: 32537350
- PMCID: PMC7253278
- DOI: 10.1097/GOX.0000000000002694
Indocyanine Green Angiography in Breast Reconstruction: Utility, Limitations, and Search for Standardization
Abstract
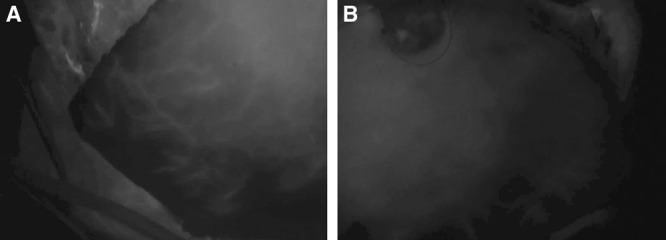
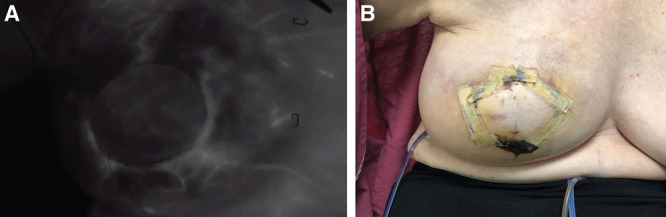
During reconstructive breast surgery, intraoperative assessment of tissue perfusion has been solely based on subjective clinical judgment. However, in the last decade, intraoperative indocyanine green angiography (ICGA) has become an influential tool to visualize blood flow to the tissue of interest. This angiography technique produces real-time blood flow information to provide an objective assessment of tissue perfusion.
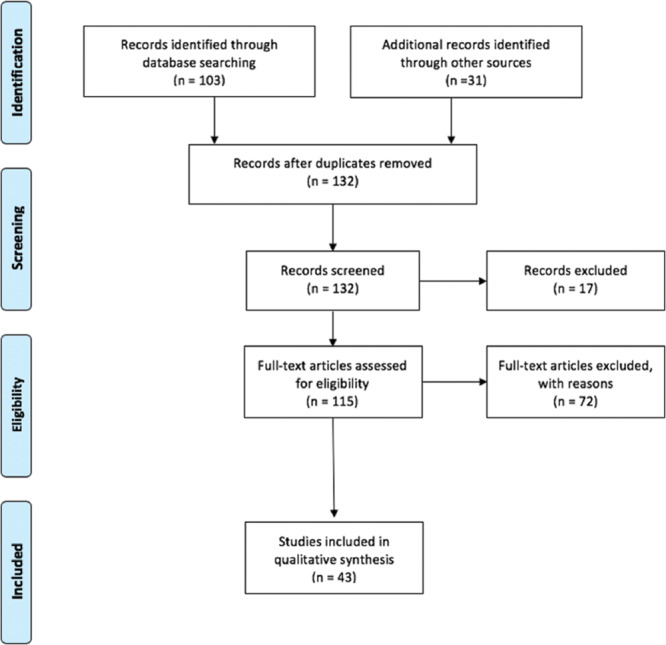
Methods: A comprehensive literature search of articles pertaining to ICGA in breast reconstruction surgery was performed. The overall findings of the articles are outlined here by surgical procedure: skin-sparing and nipple-sparing mastectomy, implant-based reconstruction, and autologous reconstruction.
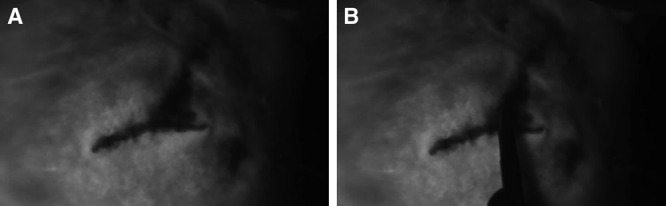
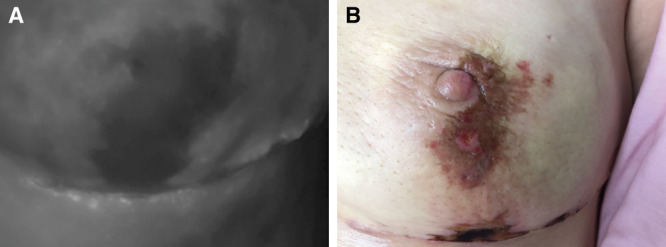
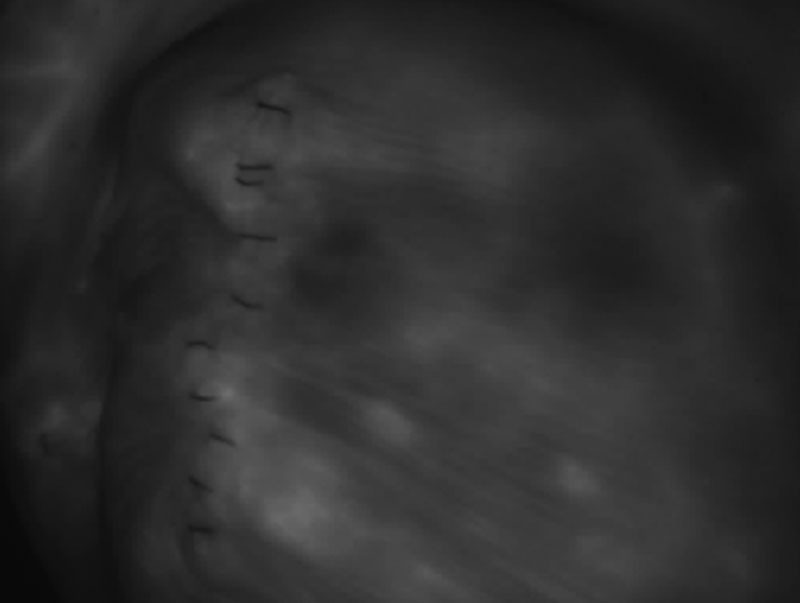
Results: Overall, there were 133 articles reviewed, describing the use of ICGA in breast reconstruction surgery. We found that ICGA can provide valuable information that aids in flap design, anastomotic success, and perfusion assessment. We also included example photographs and videos of ICGA use at our institution.
Conclusions: ICGA can reduce postoperative tissue loss and aid in intraoperative flap design and inset. Despite the benefits of ICGA, its technical use and interpretation have yet to be standardized, limiting its widespread acceptance.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Figures
Similar articles
-
Tailoring through Technology: A Retrospective Review of a Single Surgeon's Experience with Implant-Based Breast Reconstruction before and after Implementation of Laser-Assisted Indocyanine Green Angiography.Breast J. 2016 May;22(3):274-81. doi: 10.1111/tbj.12576. Epub 2016 Feb 21. Breast J. 2016. PMID: 26899399 Clinical Trial.
-
Does the Use of Intraoperative Angiography Reduce the Incidence of Postoperative Wound and Flap Complications in Complex Lower Extremity Oncologic Reconstruction?Ann Plast Surg. 2021 Jul 1;87(1s Suppl 1):S13-S16. doi: 10.1097/SAP.0000000000002800. Ann Plast Surg. 2021. PMID: 33833180
-
Evaluation of Intraoperative Anastomotic Patency with Angiography in Microsurgical Breast Reconstruction.Plast Reconstr Surg Glob Open. 2023 Sep 6;11(9):e5230. doi: 10.1097/GOX.0000000000005230. eCollection 2023 Sep. Plast Reconstr Surg Glob Open. 2023. PMID: 37681066 Free PMC article.
-
The Utility of Indocyanine Green Angiography in Breast Reconstruction to Detect Mastectomy Skin Flap Necrosis and Free Flap Perfusion: An Umbrella Review.Bioengineering (Basel). 2024 Oct 15;11(10):1025. doi: 10.3390/bioengineering11101025. Bioengineering (Basel). 2024. PMID: 39451401 Free PMC article. Review.
-
Optimizing Indocyanine Green Fluorescence Angiography in Reconstructive Flap Surgery: A Systematic Review and Ex Vivo Experiments.Surg Innov. 2020 Feb;27(1):103-119. doi: 10.1177/1553350619862097. Epub 2019 Jul 26. Surg Innov. 2020. PMID: 31347468
Cited by
-
Normalization of Time-Intensity Curves for Quantification of Foot Perfusion Using Near-Infrared Fluorescence Imaging With Indocyanine Green.J Endovasc Ther. 2023 Jun;30(3):364-371. doi: 10.1177/15266028221081085. Epub 2022 Mar 3. J Endovasc Ther. 2023. PMID: 35236169 Free PMC article.
-
Indocyanine Green Angiography to Predict Complications in Subcutaneous Mastectomy: A Single-Center Experience.J Pers Med. 2025 Jun 10;15(6):242. doi: 10.3390/jpm15060242. J Pers Med. 2025. PMID: 40559105 Free PMC article.
-
Mastectomy Skin Flap Perfusion Assessment Prior to Breast Reconstruction: A Narrative Review.J Pers Med. 2024 Sep 6;14(9):946. doi: 10.3390/jpm14090946. J Pers Med. 2024. PMID: 39338200 Free PMC article. Review.
-
Advances in Prepectoral Breast Reconstruction.Ther Clin Risk Manag. 2023 Apr 18;19:361-368. doi: 10.2147/TCRM.S404799. eCollection 2023. Ther Clin Risk Manag. 2023. PMID: 37095832 Free PMC article. Review.
-
Using ICG to Streamline Perforator Selection in DIEP Flap Reconstruction: Retrospective cohort study of outcomes in our first one hundred flaps.JPRAS Open. 2025 Mar 6;44:331-338. doi: 10.1016/j.jpra.2025.02.016. eCollection 2025 Jun. JPRAS Open. 2025. PMID: 40276248 Free PMC article.
References
-
- Khavanin N, Qiu C, Darrach H, et al. Intraoperative perfusion assessment in mastectomy skin flaps: how close are we to preventing complications? J Reconstr Microsurg. 2019;35:471–478. - PubMed
-
- Liu DZ, Mathes DW, Zenn MR, et al. The application of indocyanine green fluorescence angiography in plastic surgery. J Reconstr Microsurg. 2011;27:355–364. - PubMed
-
- Reinhart MB, Huntington CR, Blair LJ, et al. Indocyanine green: historical context, current applications, and future considerations. Surg Innov. 2016;23:166–175. - PubMed
-
- Duggal CS, Madni T, Losken A. An outcome analysis of intraoperative angiography for postmastectomy breast reconstruction. Aestet Surg J. 2014;34:61–65. - PubMed
LinkOut - more resources
Full Text Sources