

Secondary analyses to assess the profound effects of empagliflozin on endothelial function in patients with type 2 diabetes and established cardiovascular diseases: The placebo-controlled double-blind randomized effect of empagliflozin on endothelial function in cardiovascular high risk diabetes mellitus: Multi-center placebo-controlled double-blind randomized trial
- PMID: 32537887
- PMCID: PMC7610132
- DOI: 10.1111/jdi.13289
Secondary analyses to assess the profound effects of empagliflozin on endothelial function in patients with type 2 diabetes and established cardiovascular diseases: The placebo-controlled double-blind randomized effect of empagliflozin on endothelial function in cardiovascular high risk diabetes mellitus: Multi-center placebo-controlled double-blind randomized trial
Abstract
Aims/introduction: Recent clinical trials on sodium-glucose cotransporter 2 inhibitors showed improved outcomes in patients with type 2 diabetes at a high risk of cardiovascular events. However, the underlying effects on endothelial function remain unclear.
Materials and methods: The effect of empagliflozin on endothelial function in cardiovascular high risk diabetes mellitus: Multi-center placebo-controlled double-blind randomized (EMBLEM) trial in patients with type 2 diabetes and cardiovascular disease showed empagliflozin treatment for 24 weeks had no effect on peripheral endothelial function measured by reactive hyperemia peripheral arterial tonometry. This post-hoc analysis of the EMBLEM trial included a detailed evaluation of the effects of empagliflozin on peripheral endothelial function in order to elucidate the clinical characteristics of responders or non-responders to treatment.
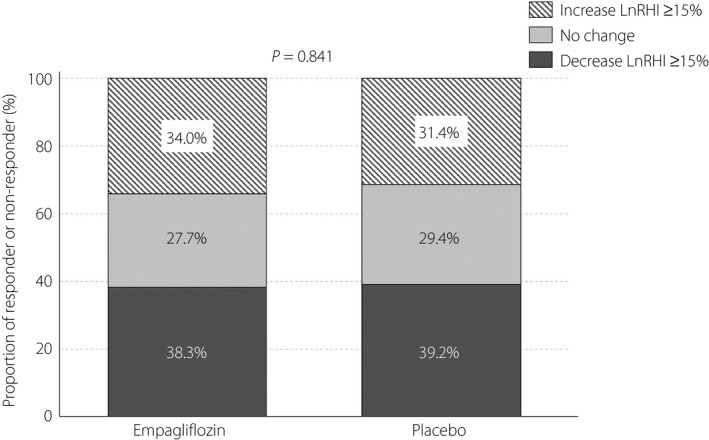
Results: Of the 47 patients randomized into the empagliflozin group, 21 (44.7%) showed an increase in the reactive hyperemia index (RHI) after 24 weeks of intervention, with no apparent difference in the clinical characteristics between patients whose RHI either increased (at least >0) or did not increase. There was also no obvious difference between the treatment groups in the proportion of patients who had a clinically meaningful change (≥15%) in log-transformed RHI. No correlation was found between changes in RHI and clinical variables, such as vital signs and laboratory parameters.
Conclusions: Treatment with empagliflozin for 24 weeks in patients with type 2 diabetes and cardiovascular disease did not affect peripheral endothelial function, and was not related to changes in clinical variables, including glycemic parameters. These findings suggest that the actions of sodium-glucose cotransporter 2 inhibitors other than direct improvement in peripheral endothelial function were responsible, at least in the early phase, for the clinical benefits found in recent cardiovascular outcome trials.
Keywords: Cardiovascular disease; Empagliflozin; Endothelial function.
© 2020 The Authors. Journal of Diabetes Investigation published by Asian Association for the Study of Diabetes (AASD) and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
AT received modest honoraria from Astellas, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Fukuda Denshi, Kowa, Merck, Mitsubishi Tanabe, Novo Nordisk, Taisho Toyama, Takeda and Teijin; and a research grant from GlaxoSmithKline. MS received honorarium and an endowed chair from Boehringer Ingelheim. HT received lecture fees from Bayer, Boehringer Ingelheim, Daiichi Sankyo, Kowa, Takeda, Mitsubishi Tanabe and Sanwa Kagaku Kenkyusho. YO received lecture fees from Astellas, AstraZeneca, MSD, Ono, Mitsubishi Tanabe, Bayer, Novo Nordisk, Eli Lilly, Boehringer Ingelheim, Daiichi Sankyo, Kissei, Novartis, Kowa and Sanwa Kagaku Kenkyusho; and research funds from Kowa and Mitsubishi Tanabe. TT received honoraria from MSD, Astellas, AstraZeneca, Mitsubishi Tanabe, Boehringer Ingelheim, Novo Nordisk and Taisho Toyama; research funding from Kowa; and scholarships from Novartis, AstraZeneca, Astellas and Novo Nordisk. MY‐T received honoraria from Bayer, Mitsubishi Tanabe, Itamar, MSD, Nippon Shinyaku, Boehringer Ingelheim and Daiichi Sankyo. SU received research grants from Bristol‐Myers Squibb and Kowa; non‐purpose research grants from Bristol‐Myers Squibb, Chugai, MSD, Pfizer and Takeda; and lecture fees from Boehringer Ingelheim and MSD. YH received consulting fees from Mitsubishi Tanabe related to this study, as well as honoraria and grants from Teijin, Boehringer Ingelheim, MSD, Sanofi, AstraZeneca, Kyowa Hakko Kirin, Takeda, Astellas, Daiichi Sankyo, Mochida, Nihon Kohden, Shionogi, Nippon Sigmax, Sanwa Kagaku Kenkyusho, Unex and Kao; and honoraria from Radiometer, Omron, Sumitomo Dainippon, Otsuka, Torii, Kowa, Fujiyakuhin, Amgen, Nippon Shinyaku, Itamar, Bayer, Eli Lilly and Ono. KN received honoraria from Eli Lilly, Astellas, Ono, Takeda, Daiichi Sankyo, Boehringer Ingelheim, MSD, Mitsubishi Tanabe, AstraZeneca; research grants from Amgen, Teijin, Terumo, Mitsubishi Tanabe, Asahi Kasei, Astellas, Boehringer Ingelheim and Bayer; and scholarships from Bayer, Daiichi Sankyo, Teijin, Astellas, Takeda and Bristol‐Myers Squibb. The other authors declare no conflict of interest.
Figures

References
-
- Heerspink HJ, Perkins BA, Fitchett DH, et al Sodium glucose cotransporter 2 inhibitors in the treatment of diabetes mellitus: cardiovascular and kidney effects, potential mechanisms, and clinical applications. Circulation 2016; 134: 752–772. - PubMed
-
- Tanaka A, Node K. Emerging roles of sodium‐glucose cotransporter 2 inhibitors in cardiology. J Cardiol 2017; 69: 501–507. - PubMed
-
- Zinman B, Wanner C, Lachin JM, et al Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015; 373: 2117–2128. - PubMed
-
- Neal B, Perkovic V, Mahaffey KW, et al Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017; 377: 644–657. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
